TODAY'S CHIROPRACTIC , November 2000
by Erin Elster, DC.
INTRODUCTION
Multiple Sclerosis (MS) is the foremost disabling neurological disease among adults between 20 and 50 years of age, afflicting 250,000 people in the United States. (1) It strikes women twice as often as men and Caucasians more frequently than other ethnic groups. (1) The occurrence of MS is greater in northern temperate zones. (1)
The pathological process involved in MS, a demyelinating disease, is the loss of the myelin sheaths surrounding axons in the central nervous system. Demyelination is thought to result either from damage to the oligodendrocytes (white matter cells) that produce the myelin or from a direct, immunologic (auto-immune) assault on the myelin itself. (2)
Common early manifestations of MS include paresthesias (numbness/tingling in extremities), optic neuritis (vision loss), mild sensory or motor symptoms in a limb, and cerebellar incoordination (balance loss). Although the most common course of the condition is a relapsing and remitting pattern over many years, the manifestation in each patient varies. In most cases, as the disease progresses, remissions become less complete. Some patients have only a few brief episodes of disability, whereas others have a relentless downhill course over months or weeks. Although not all patients become disabled, the end stage often can include ataxia (inability to coordinate voluntary movement), incontinence, paraplegia, and mental dysfunction due to widespread cerebral and spinal cord demyelination. (2)
The MS diagnosis, primarily a clinical one, is usually rendered based on neurological history and examination. The diagnosis can be confirmed by specialized evaluation techniques including magnetic resonance imaging (MRI), evoked potentials, and cerebrospinal fluid (CSF) analysis, although none show findings pathognomonic for MS. (3-5) Traditional medical treatment for MS focuses on the use of medications to regulate the severity of symptoms such as depression, pain, bladder impairment, and sexual dysfunction. Other drugs may accelerate recovery from acute exacerbations of MS, but they neither alter the long-term course of the condition nor reverse any existing MS symptoms. (6)
B.J. Palmer, D.C., reported management of Multiple Sclerosis patients with upper cervical chiropractic care as early as 1934. (7-8) In his writings, Palmer listed improvement or correction of symptoms such as "spasticity, muscle cramps, muscle contracture, joint stiffness, fatigue, neuralgia, neuritis, loss of bladder control, paralysis, incoordination, trouble walking, numbness, pain, foot drop, inability to walk, and muscle weakness." His chiropractic care included paraspinal thermal scanning using a neurocalometer (NCM), a cervical radiographic series to analyze injury to the upper cervical spine, and a specific upper cervical adjustment performed by hand.
While few of Palmer's Research Clinic cases were published, Palmer described one case of Multiple Sclerosis in detail. (8) The patient, a 38-year-old male, went to the Palmer Research Clinic in Davenport, Iowa, in 1943, after a diagnosis of MS by the Mayo Clinic. At the time of admission into the Palmer Clinic, this subject was "…helpless; he could not feed nor take care of himself." His medical history included a head/neck trauma at age 16 in which "…he fell ten feet off a building, landing on his head." The fall rendered him unconscious for thirty minutes and he reported having a sore neck for several days. At the Palmer Clinic, upper cervical radiographs showed a misalignment of the atlas to the right. After upper cervical chiropractic care, the patient remarked, "I am happy to say that through chiropractic, I have been made almost well. Today, I have just a little numbness left in my hands. I have the full use of my hands, feet, and my whole body."
During the past several decades, research linking chiropractic and MS has been virtually nonexistent. A literature search produced only two single case reports. One patient was adjusted with an instrument, while the other was managed with thoracolumbar manual chiropractic adjusting procedures. (9-10) No other references for the chiropractic management of MS patients were found. To the author's knowledge, the MS cases discussed in this report are the first documented using specific upper cervical care (cervical radiographs, thermal imaging, and knee-chest adjustments) since Palmer's research seventy years ago.
The following five individuals suffered from Multiple Sclerosis for one to ten years, ranged from 33 to 55 years of age, and had symptoms varying from mild to severe. All patients showed lesions on MRI (MS plaques) and were diagnosed with MS by their neurologist. Some concurrently were undergoing treatment with medications. The following report discusses the upper cervical chiropractic intervention in detail and summarizes the five cases' results.
IUCCA UPPER CERVICAL CHIROPRACTIC INTERVENTION
At each subject's first upper cervical chiropractic office visit, her/his medical history was discussed. In Case 1, a nine-year history of the typical relapsing-remitting pattern of MS symptoms was established. In Cases 2 through 5, MS symptoms were constant and progressively worsening without remission
Paraspinal digital infrared imaging, which measures cutaneous infrared heat emission, was chosen as the diagnostic test for neurophysiology. Thermography has been proven valid as a neurophysiological diagnostic imaging procedure with over 6000 peer-reviewed and indexed papers in the past 20 years. In blind studies comparing thermographic results to that of CAT scans, MRI, EMG, myelography, and surgery, thermography was shown to have a high degree of sensitivity (99.2%), specificity (up to 98%), predictive value, and reliability. (11-13) Thermal imaging has been effective as a diagnostic tool for breast cancer, repetitive strain injuries, headaches, spinal problems, TMJ conditions, pain syndromes, arthritis, and vascular disorders, to name a few. (14-23)
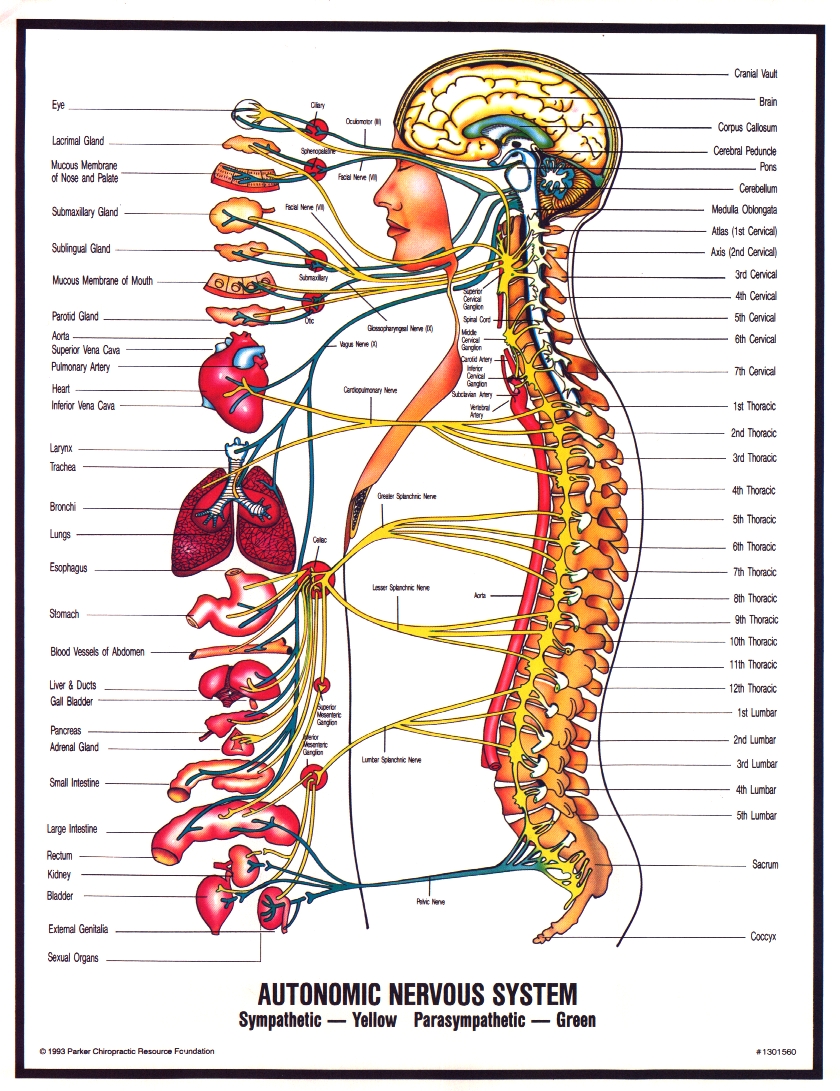
At each patient's first upper cervical chiropractic office visit, a paraspinal thermal analysis was performed from the level of C7 to the occiput according to thermographic protocol. (24-26) Compared to established normal values for the cervical spine, each of the five subject's paraspinal scans contained thermal asymmetries higher than 0.5 ºC. According to cervical thermographic guidelines, thermal asymmetries of 0.5ºC or higher indicate abnormal autonomic regulation or neuropathophysiology. (27-30) Because upper cervical misalignments were suspected in all five patients, a precision upp
er cervical radiographic series, including Lateral, A-P, A-P Open Mouth, and Base Posterior views, was performed at each patient's initial chiropractic office visit. (31) These four views enabled examination of the upper cervical spine in three dimensions: sagittal, coronal, and transverse. To maintain postural integrity, each subject was placed in a positioning chair using head clamps. Analysis of the four views was directed towards the osseous structures (foramen magnum, occipital condyles, atlas, and axis) that are intimately associated with the neural axis. Laterality and rotation of atlas and axis were measured according to each vertebra's deviation from the neural axis. (31) All five patients showed upper cervical misalignments.
Because the two criteria determining subluxation (thermal asymmetry and vertebral misalignment) were met in each case, a treatment plan was discussed with each patient. After each subject consented, chiropractic care began with an adjustment to correct the atlas/axis misalignment. To administer the adjustment, the patient was placed on a knee-chest table with his/her head turned to the direction of misalignment (left for left misalignments and right for right misalignments). The knee-chest posture was chosen because of the accessibility of the anatomy to be corrected. In addition, this posture retained spinal curvatures, thus preventing compression of the spine. Using the posterior arch of atlas as the contact point, an adjusting force was introduced by hand. (32) The adjustment's force (force = mass X acceleration) was generated using body drop (mass) and a toggle thrust (acceleration).
Then, each patient was placed in a post-adjustment recuperation suite for fifteen minutes as per thermographic protocol. (24-26) The adjustment's success was determined by reviewing the post-adjustment thermal scan. The first post-adjustment scans of all five patients revealed thermal differences of 0.1 ºC to 0.2ºC, which were considered normal according to established cervical thermographic guidelines (compared to the pre-adjustment differential of 0.5 ºC or greater). Therefore, resolution of each patient's presenting thermal asymmetry was achieved.
All subsequent office visits for each patient began with a thermal scan. An adjustment was administered only when the patient's presenting thermal asymmetry returned. If an adjustment was given, a second scan was performed after a fifteen-minute recuperation period to determine whether restoration of normal thermal symmetry had occurred. On average, each subject's office visits occurred three times per week for the first two weeks of care, two times per week for the following two weeks, and once per week for the subsequent month. After spinal stability was achieved (thermal asymmetry was rarely present), visits were reduced to once per month.
CASE 1
History: This 54-year-old female was diagnosed with Multiple Sclerosis at age 44 after a bout of optic neuritis, which prompted an MRI (MS plaques were visible). Over the next nine years, she experienced a minimum of one exacerbation per year lasting an average of one month. She recovered completely each time except for partial vision loss resulting from optic neuritis. The most recent flare-up occurred at age 53 when she experienced numbness that switched from side-to-side in her body. With this exacerbation, no remission occurred. Symptoms included tingling in her arms, hands, legs, and feet as well as a positive L'hermitte's Sign (pain, numbness, tingling down extremities upon cervical flexion). After these symptoms were present for three months, this subject's neurologist surmised her condition was worsening and recommended drug therapy. Due to her concerns over long-term drug use, this patient chose to undergo upper cervical chiropractic care first.
Exam: During her initial chiropractic examination, this subject showed reduced sensitivity bilaterally in her arms, hands, legs, and feet. L'hermitte's Sign was present during cervical flexion and right lateral flexion compression was positive. The subject reported experiencing these symptoms constantly for the three months prior to her chiropractic exam. Cervical ranges of motion were reduced during left lateral bending and left rotation. She reported visual loss from previous optic neuritis episodes. Computerized thermal imaging showed thermal asymmetries as high as 1.0 ºC. Analysis of cervical radiographs revealed left laterality and left anterior rotation of atlas.
Outcome: Immediately following this subject's first upper cervical adjustment, Lhermitte's Sign was no longer present. During the following week, normal sensation returned to her extremities. After two weeks of upper cervical care, cervical ranges of motion no longer produced pain and cervical compression tests were negative. At the end of week four, this patient reported improved vision in her left eye (which had been damaged by the episode of optic neuritis ten years earlier). After four weeks of upper cervical care, this subject's neurologist reexamined her and no longer recommended drug therapy. Two years after beginning upper cervical care, this subject remained symptom-free.
Summary: This patient experienced a minimum of one relapse per year for the ten years prior to upper cervical care. After upper cervical intervention, two years passed without reoccurrence of symptoms.
CASE 2
History: After this 33-year-old male noticed visual changes at age 30, he was examined by a neuro-opthalmologist and showed 20/30 vision in the right eye (according to the Snellen eye chart examination). After an MRI showed three brain lesions (MS plaques), he was diagnosed with MS. The year following his diagnosis, this subject showed minimal deterioration in his condition. However, during the subsequent two years, he experienced chronic progression of MS symptoms. In addition to vision loss, he suffered from loss of bladder control, constipation, loss of balance, sensory deficits in his extremities, and L'hermitte's sign. Three years after the MS diagnosis, he was reexamined by his neuro-opthalmologist who noted his optic nerves appeared pale and his vision had deteriorated to 20/400 in the right eye and 20/200 in the left eye. He was declared legally blind. A follow-up MRI showed ten lesions, one active. This subject began upper cervical care soon after the second MRI.
Exam: During this patient's initial examination, he reported wearing sunglasses at all times, even indoors, due to light sensitivity. L'hermitte's Sign was present. Sensitivity was reduced in his hands and feet. Heat aggravated his symptoms. He showed inability to balance on one foot bilaterally and to walk heel-to-toe in a straight line. As a result, he reported frequent falls on hiking trails. He reported difficulty with bladder control (he urinated six times per night) and constipation (averaging four to five days without a bowel movement). He also suffered with memory loss (he carried a tape recorder to remind himself of errands, etc.), insomnia, and fatigue. Most of his MS symptoms had progressively worsened during the second and third years following his diagnosis and had been constant for at least one year. Analysis of cervical radiographs revealed left laterality of atlas. Computerized thermal imaging showed thermal asymmetries as high as 0.8ºC.
Outcome: After the first upper cervical adjustment, L'hermitte's Sign was absent and balancing on his left leg improved (both symptoms had been present for one year or greater). One week later, he reported that due to less light sensitivity, he was able to leave his sunglasses off, even outdoors. Upon visual reexamination one month later, he tested 20/160 bilaterally. Six months later, balancing on both left and right legs improved, so he was able to resume hiking while carrying a heavy backpack. He also was able to take hot showers and sit in jacuzzis because heat no longer aggravated his symptoms. In addition, normal sensation returned to his extremities, bladder control improved (urination occurred once per night), and constipation improved (one bowel movement per day).
Summary: During the two years prior to chiropractic care, this patient experienced a progressive worsening of MS symptoms. Most symptoms had been present constantly for at least one year prior to the start of upper cervical care. After the intervention of chiropractic care, this subject reported immediate correction of some symptoms as well as gradual improvement of other symptoms over several months. One year after beginning care, this patient reported an overall correction and/or improvement in MS symptoms.
CASE 3
History: This 46-year-old female first experienced symptoms of MS at age 44, when she noticed memory and cognitive problems (inability to formulate thoughts or words), frequent urination and loss of bladder control (loss of muscular control to begin and end urination). She was diagnosed with MS after an MRI showed active brain lesions. Her symptoms remained constant without worsening until the addition of sensory deficits (painful tingling) in her arms and legs, two years after her diagnosis.
Exam: At her initial chiropractic examination, this subject reported feeling continuous, painful tingling and loss of sensation in both arms and legs during the previous month. She complained of a weakness in her legs that she described as "a rubbery feeling." She also had difficulty with cognition and bladder control for the previous two years. She complained of generalized stiffness and aching in her neck. Cervical extension was reduced and painful. Analysis of cervical radiographs revealed right laterality and right posterior rotation of atlas. Computerized thermal imaging showed 0.5ºC thermal asymmetries.
Outcome: Within the first week of upper cervical care, this subject reported improved bladder control (resumption of muscular control during urination) and a decrease in numbing, tingling, and pain in her left leg and right hand. One month later, her leg strength returned and numbness was noted only in her left hand. In addition, memory and cognitive ability returned to normal. After two months of care, bladder control, sensitivity, and strength in her extremities returned to normal. After four months of upper cervical care, this subject reported the absence of all MS symptoms. A follow-up MRI showed no new lesions as well as a reduction in intensity of the original lesions. During the subsequent six months, this patient was examined once per month with digital infrared imaging. An adjustment was necessary on three visits. At each of those three occasions, a minor reoccurrence of symptoms also existed, which was corrected following each adjustment. No other flare-ups occurred.
Summary: Most of this patient's MS symptoms (except one month of sensory deficits) had been present for two years prior to the start of upper cervical care. After the intervention of upper cervical chiropractic care, the patient's MS symptoms gradually improved over several months. After one year of care, this individual primarily remained asymptomatic.
CASE 4
History: This 55-year-old female was diagnosed with MS nine years ago at age 46 after an MRI confirmed active brain lesions. Her symptoms included painful paresthesia of her left arm, fatigue, mental confusion, insomnia, and lack of coordination of her right arm and leg. All symptoms progressively worsened over the nine-year period. Seven years after her diagnosis, a follow-up MRI confirmed the addition of new active lesions. Due to the fatigue, confusion, and pain, she had been on disability leave from work for several years.
Exam: During this patient's initial exam, she complained of extreme pain in her left arm, requiring multiple doses per day of pain medication (neurontin). She also took daily medication for sleeping (klonopin) and energy level (amantadine) due to her insomnia and fatigue. Her handwriting coordination (right-handed) was poor so she preferred using a computer. Cervical radiographs depicted a misalignment of her atlas to the right and posterior. Computerized thermal imaging revealed thermal asymmetries of 0.5ºC.
Outcome: During the first week of upper cervical care, this subject noticed an increase in energy level. One month later, she no longer noticed arm pain. Consequently, she consulted with her neurologist to reduce her pain medication. Her pain medication was reduced by two-thirds and she had no occurrences of arm pain. This patient also reported a continued increase in energy level and a renewed sense of mental clarity, so she considered looking for a part-time job. She felt "more alert and energized" and her "mind was clear." Four months after the start of upper cervical care her condition continued to improve without any relapses.
Summary: For the nine years prior to upper cervical care, this patient suffered from a chronic, progressive worsening of MS symptoms. Since the intervention of upper cervical care, this individual experienced improvements in MS symptoms and required less medication.
CASE 5
History: This 43-year-old female first experienced symptoms of MS seven years ago. The symptoms included numbness in her legs, hands, and face, and lasted for two weeks. No further symptoms occurred until six years later with the onset of L'hermitte's Sign. Soon after L'hermitte's Sign began, this patient noticed loss of grip strength and a spasmodic curling of her left hand. After an MRI, she was diagnosed with MS. Because Lhermitte's Sign was present every time she nodded her head causing her pain, she began daily pain medications (neurontin). After the symptoms were constantly present for six months, she began upper cervical care.
Exam: During her initial chiropractic exam, cervical flexion produced L'hermitte's Sign. Cervical extension and left rotation were reduced and painful. She reported constant tingling in her left arm, grip strength loss in her left hand, and weakness and pain in both forearms. She experienced aggravation of forearm pain while taking notes in class. As an avid martial arts participant, she expressed concern over her inability to perform push-ups in class due to exacerbation of L'hermitte's Sign. She also reported experiencing dizzy spells several times per day for many years. Cervical radiographs depicted right laterality of atlas. Computerized thermal imaging revealed thermal asymmetries of 0.5ºC.
Outcome: After the first upper cervical adjustment, this patient noted reduction in intensity of L'hermitte's Sign. By the end of two weeks of care, L'hermitte's Sign was noticeable only occasionally and no dizzy spells had occurred. After four weeks of care, this patient no longer reported experiencing any dizzy spells, arm pain, tingling, forearm weakness, or L'hermitte's Sign. Consequently, she reduced her pain medication dosage. In addition, she resumed taking notes in class and performing pushups in her martial arts class without pain or tingling.
Summary: This subject's symptoms were present constantly for six months prior to upper cervical care. With the intervention of chiropractic care, symptoms were reversed either immediately or over one month's time.
RESULTS
At their first upper cervical chiropractic office visits, computerized thermal scans showed thermal asymmetries and cervical radiographs showed upper cervical misalignments in all five subjects. Because these exam findings indicated upper cervical injuries, all five patients consented to upper cervical chiropractic care. The five subjects underwent upper cervical care for a minimum of four months and a maximum of two years at the time of this paper's submission for publication. Before the intervention of upper cervical chiropractic care, four out of the five patients (Cases 2 through 5) showed patterns of constant, progressive MS symptoms for a minimum of six months. After upper cervical care, MS symptoms were improved or corrected, including L'hermitte's Sign, paresthesias, pain, balance, muscle weakness, bladder control, bowel control, cognitive ability, vision loss, insomnia, dizziness, and fatigue. The only case that followed the typical MS relapse-remit pattern, Case 1, had a history of MS relapses once per year for nine years. After the intervention of upper cervical care, this subject had no further relapses and remained symptom-free for two years. Therefore, results of the five cases indicated that upper cervical chiropractic care prevented the progression of MS, stopped the MS relapse pattern, and improved and/or reversed symptoms of
DISCUSSION
An important parallel in the MS patients' medical histories was their recollection of head and/or neck trauma(s) prior to the onset of MS (also mentioned in the Palmer case described in the Introduction). All five patients remembered specific incidences of trauma preceding the onset of MS symptoms such as a fall on an icy sidewalk, an auto accident, and a ski accident. In addition, all five individuals showed evidence of upper cervical injury during exams (digital infrared imaging and cervical radiographs). The body of medical literature detailing a possible trauma-induced etiology for MS, or at least a contribution, is substantial. (33-35) In fact, medical research has established a connection between spinal trauma and numerous neurological conditions besides Multiple Sclerosis, including Parkinson's Disease, Amyotrophic Lateral Sclerosis (ALS), epilepsy, migraine headaches, Attention Deficit Hyperactivity Disorder (ADHD), vertigo, and bipolar disorder, to name a few. (36-43)
While medical research has shown that trauma may lead to MS and the other neurological conditions mentioned above, no mechanism has been defined. It is the author's hypothesis that the missing link may be the injury to the upper cervical spine. While various theories have been proposed to explain the effects of chiropractic adjustments, a combination of several theories seems most likely to explain the profound changes seen in these MS patients due to upper cervical chiropractic care. After a spinal injury, central nervous system (CNS) facilitation can occur from an increase in afferent signals to the spinal cord and/or brain coming from articular mechanoreceptors. (44-48) The upper cervical spine is uniquely suited to this condition because it possesses inherently poor biomechanical stability along with the greatest concentration of spinal mechanoreceptors.
Hyperafferent activation (through CNS facilitation) of the sympathetic vasomotor center in the brainstem and/or the superior cervical ganglion may lead to changes in cerebral blood flow, including ischemia. (49-55) Because of the close association between the nervous and immune systems (the immune system recently has been reclassified as the neuroimmune system), upper cervical injuries affecting sympathetic function consequently may cause a cascade of non-favorable immune responses. (56-58) Among these are uncoordinated immune tissue responses (auto-immune responses) and the release of cortisol, which ultimately can result in decreased immune function.
It is likely that the five MS patients sustained injuries to their upper cervical spines (visualized on cervical radiographs) during spinal traumas they experienced. It is also likely that due to the injuries, through the mechanisms described previously, sympathetic malfunction occurred (measured by paraspinal digital infrared imaging), possibly causing decreases in cerebral blood flow. Consequently, because the nervous and immune systems are so closely intertwined, it is possible that CNS facilitation and cerebral ischemia could have stimulated an auto-immune response such as myelin destruction. According to the results of each of the five patients discussed in this report, it seems correction of the upper cervical injury not only stopped but also reversed the pathological processes involved in MS. However, few conclusions can be drawn from a small number of cases. Therefore, further research is recommended to study the link between trauma, the upper cervical spine, and neurological disease.
CONCLUSION
All five patients discussed in this report recalled experiencing head or neck trauma(s) prior to the onset of Multiple Sclerosis symptoms. In all five cases, evidence of upper cervical injury was found using paraspinal digital infrared imaging and upper cervical radiographs. After IUCCA upper cervical chiropractic care, all five cases reviewed revealed improvements in Multiple Sclerosis symptoms. In fact, correction of the five patients' upper cervical injuries appeared to stimulate a reversal in the progression of MS symptoms. To the author's knowledge, these are the first cases reported on this topic using thermal imaging and knee-chest adjustments since Palmer's research seventy years ago. Further investigation into upper cervical injury and resulting neuropathophysiology as a possible etiology or contributing factor to Multiple Sclerosis should be pursued.


 A recent journal study was the first to reveal that correction of upper neck injuries might help improve or even reverse the progression of Multiple Sclerosis (MS) and Parkinson's disease (PD).
A recent journal study was the first to reveal that correction of upper neck injuries might help improve or even reverse the progression of Multiple Sclerosis (MS) and Parkinson's disease (PD). 



.jpg)
