THE ANATOMY OF THE ATLAS SUBLUXATION
The atlas subluxation is so common yet so easily missed by mainstream medical practitioners. This problem is not very difficult to detect, in fact my daughter has become quite adept at picking out people walking down the street who exhibit the hallmarks of this upper cervical subluxation. There are maybe two reasons why most medical doctors do not detect this phenomenon. One could be that they doubt completely the existence of such subluxations and the other is maybe that their training is focussed on looking for major problems like dislocations, fractures, tumours and the like. The purpose of this section is to summarise what an atlas subluxation looks like and what actually happens to one's body when one does sustain such a misalignment of one's atlas. There is a wealth of information in medical texts, on websites and in scientific papers that provide more in-depth information. Hopefully, my summary will assist the layperson to understand the phenomenon, which is "the atlas subluxation".
The term 'subluxation' means 'minor misalignment' however the affects on the human body as a result of a subluxation of the first cervical vertebra (C1 or atlas) with respect to the skull can be far from 'minor'. To understand what the 'anatomy of an atlas subluxation' looks like it's first important to understand the anatomy of the atlas. The following graphic depicts the atlas (C1) vertebra articulating with the axis (C2) vertebra below it. The spinal cord with exiting spinal nerves can be seen tethered by dentate ligaments to the inner margins of the vertebral foramen. The human skull via the occipital condyles at the base of the skull sits on top of (or articulates with) the superior articular condylar surface of the atlas. According to Gray's Anatomy[1] "This articulation is a double condyloid joint. Its ligaments are the Anterior Occipito-atlantal, Posterior Occipito-atlantal, two Lateral Occipital-atlantal and two Capsular." There is a passage on each side in the Posterior Occipito-atlantal ligament to allow penetration of the vertebral arteries and 1st cervical nerves. The vertebral arteries exit the foramen in the atlas transverse processes; penetrate the ligament and then loop up into the brain. A number of strong ligaments support the skull and its contents and attach it to the cervical spine. Many other ligaments and muscles enable movement, bending, twisting and head rotation. There are other key structures within the vicinity of the atlas and supporting ligaments. These are 4 pairs of cranial nerves, namely the vagus, spinal accessory, glossopharyngeal and hypoglossal. The common carotid arteries, which run underneath the sternocleidomastoid muscle and jugular veins, are also present in the tissues of the neck. At the base of the neck near the junction of the shoulders there are some deep muscles known as the scalenes. These are the posterior, middle and anterior scalenes. The anterior scalenes are of particular interest as they are in very close proximity to the brachial plexus of nerves and the origin of the vertebral arteries where they leave the subclavian arteries. Even though the atlas is at the top of the cervical spine and the above-mentioned structures are near the base of the neck, a subluxation of the atlas and skull can result in these scalenes compressing the brachial plexus and/or the vertebral arteries. This is due to altered weight bearing from a shift in the centre of gravity of the skull, which in causes the muscles of the head and neck to strain in maintaining the head upright on the cervical spine. Also the phrenic nerve, which runs between anterior and middle scalenes on its path to the diaphragm, can be likewise affected by muscle and ligament compression and/or traction.
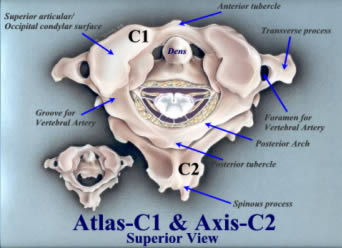
 Figure 1: Upper Cervical Spine – No subluxation
Figure 1: Upper Cervical Spine – No subluxationFigure1 opposite is a drawing of the upper cervical spine articulation between the occiput (C0), the atlas (C1) and the axis (C2). The 'usual' anatomy is for the occipital condyles (cream) of the skull to sit on the atlas condylar surfaces and for the atlas lateral masses (white) (shown cut away) to articulate with the facet joints of the axis (brown) below it. The odontoid peg or dens of the axis should sit about central to the foramen magnum. This is the front (anterior) view, if you were looking directly at the face of this person. The double condyloid joints are represented in this drawing by the 'gaps' between the occiput and atlas lateral masses.
 Figure 2: Upper Cervical Spine – Skull to atlas subluxation
Figure 2: Upper Cervical Spine – Skull to atlas subluxation Figure 2 opposite shows what can happen to the 'usual' anatomy in Figure 1, when a force is applied to the skull on one side. The blue arrow indicates the direction of trauma, which in this case is from the left side of the person's head. This trauma can take many forms. In my case it was my head striking the ground in a football tackle. For one little girl it was falling out of bed and hitting her head on the bedside table and for another lady playing basketball, it was a direct hit to the jaw. The force is enough to push the skull sideways as it slides along the atlas condylar surface. The occipital condyles of the skull can slide off (over or underlap) the atlas condylar surface, however the anatomy and the restraining ligaments limit this over and underlapping. The result in this example is a head tilted to the left, and an atlas that's high (elevated) on the right. The axis dens is no longer central to the foramen magnum. See then animation OCCIPUT TO ALTAS SUBLUXATION to view the mechanism of injury. The actual slope of the atlas condyles will determine whether or not the atlas will actually rotate a little with respect to the occiput (skull) and to the axis (C2). Flatter condyles will result in slight rotation of the atlas, whereas steep angled condyles will most likely not produce a great deal of rotation. The skull is quite heavy thus any change in the centre of gravity will most likely produce undesirable stresses on structures within the tissues of the cervical spine. This situation has important implications for the spinal cord, which leaves the foramen magnum and travels through the foramen (holes) in the atlas and other skeletal vertebrae to the base of the spine. This also has important implications for the vertebral arteries, which travel through the cervical spine from C6 to the atlas, for the carotid arteries, which travel beneath the sternocleidomastoid muscles, and for the cranial nerves leaving foramen in the skull base. All of these structures have the potential to be trapped, compressed, stretched or otherwise interfered with by the taught muscles and ligaments involved in maintaining the skull and its contents on top of the cervical spine. The resultant stresses on arteries could yield reduction in oxygenated blood flow to the brain, and on cranial nerves could result in attenuation of nervous system signals to and from the brain. The cranial nerves which are potentially involved are the vagus, spinal accessory, glossopharyngeal and hypoglossal. Of course these arteries and nerves are of major importance to proper functioning and maintenance of the human body.
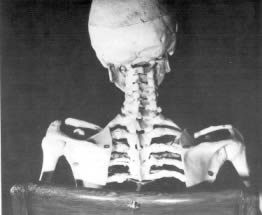 Figure 3: Even Death does not hide the proof!
Figure 3: Even Death does not hide the proof! (Source: The Chiropractic Story silently told in a medical museum – William G. Blair D.C., Ph. C., F.I.C.A., ©1973)
Copyright permission granted by Mrs Blair and Dr. E. Addington, Blair Chiropractic Clinic, Lubbock, Texas, USA.
Website: http://www.blairchiropractic.com
Figure 3 opposite is the skeleton of a soldier from the Spanish American War (1898). He developed chronic rheumatoid arthritis, the disease progressing and fusing most of his joints from his skull to his sacrum. His teeth had to be removed in order to feed him since the rheumatoid arthritis had also fused his jaw. Following his death and in accordance with his will his body was given to the Army Medical Museum. His family honoured his request and the skeleton is today displayed in the museum. Dr. William G. Blair was given permission to examine and photograph the skeleton. Figure 3, shows the head inclination as a result of a subluxation in the upper cervical spine. Since rheumatoid arthritis does not progress in death it is demonstrably obvious that the "spinal joints are fixed in the same position they occupied at the time of fusion occurred" and "since fusion can take place only in a living person, the present position of these spinal vertebra in death are the same as they were during life". These images are powerful and help to prove the existence of such subluxations of the upper cervical spine, which are the focus of specific upper cervical chiropractors like Dr. Blair and of my website. I suggest that it would be interesting indeed to hypothesise that rheumatoid arthritis is one sequelae of subluxations like this of the upper cervical spine. Fusing of joints may well be the body's way of protecting the spinal cord, brainstem and surrounding neurological and vascular structures from damage, by allowing no additional movement, which would compromise them further. Certainly it would not be the only disease process, which would be initiated if someone sustained such a condition! This injury is so high up and so close to the human central processing unit and other structures, as mentioned earlier, that it's not hard to visualise such subluxations may well be a root cause of human illness.
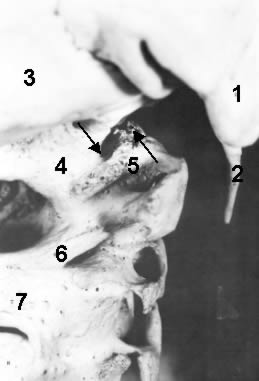 Figure 4: A close look at the subluxation!
Figure 4: A close look at the subluxation!Page 9 of Dr. Blair’s document (The Chiropractic Story silently told in a medical museum – William G. Blair D.C., Ph. C., F.I.C.A., ©1973) shows the photograph in Figure 4 opposite. Let’s have a closer look at the anatomy of this subluxation. The numbered structures are: 1. Right mastoid process; 2. Right styloid process; 3. Right side occipital bone; 4. Right occipital condyle; 5. right lateral mass of the atlas (C1); 6. Right side posterior arch of atlas; 7. Right lamina of axis (C2).
According to Blair, "You will note the fusion of all three cervical vertebrae. These vertebra are fused not only at the usual joints but also at an unusual union of the posterior arch of first cervical (6) with the right lamina of the second cervical (7). Since the growing together process can take place only in the living body, every structure is fused in the exact position it occupied during life.
Continuing our examination of Figure 4, note the two arrows. The arrow on the left points to the outside (distal) margin of the right occipital condyle (4). The arrow on the right points to the outside (distal) margin of the right lateral mass of the first cervical vertebra (5). These are the margins of the adjoining joint surfaces. Without misalignment the two arrows would line up, instead there is displacement. The first cervical vertebra is decidedly misaligned with the skull. By actual measurement on the skeleton this displacement amounts to 3/8 of an inch (approx. 1cm). The second and third cervical vertebrae have followed the first cervical vertebra to the misaligned position."
 Figure 5: An even closer look at the subluxation!
Figure 5: An even closer look at the subluxation! Page 10 of Dr. Blair's document shows these numbered structures: 1. Right mastoid process; 2. Right styloid process; 4. Right occipital condyle; 5. right lateral mass of the atlas (C1); 6. Right side posterior arch of atlas; 9. Right jaw (ramus of mandible). According to Dr. Blair, "Note the two arrows. The arrow on the left points to the front (anterior) margin of the right occipital condyle. The arrow on the right points to the front (anterior) margin of the right lateral mass of the first cervical vertebra. Again these margins are of adjoining joint surfaces. If there were no misalignment, the two arrows would line up. Again there is displacement. Again the first cervical vertebra is decidedly misaligned with the skull. The actual amount of misalignment on the skeleton is 5/8 inch (approx. 1.6cm). Also note the bony fusion of first cervical lateral mass, number 5, to the body of the second cervical vertebra below and to the occipital condyle above, number 4. These structures having grown together during life are found in exactly the same position after death as they were during life. The body of the second cervical vertebra has followed the atlas to the misaligned position and is aligned (juxtaposition) with the atlas."
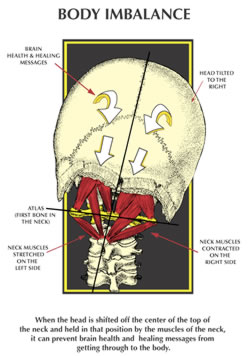 Figure 6: The Effects of the Atlas Subluxation
Figure 6: The Effects of the Atlas Subluxation(Figure 6 - reprinted with permission from Daniel O. Clark D.C., Website: www.uppercervicalillustrations.com).
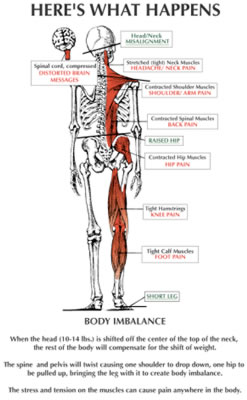 Figure 7: The Effects of the Atlas Subluxation
Figure 7: The Effects of the Atlas Subluxation(Figure 7 reprinted with permission from Daniel O. Clark D.C., Website: www.uppercervicalillustrations.com).
Figure 7 opposite explains what happens to your body if you unfortunate enough to sustain a head injury which shifts your skull on your atlas and results in a skull to atlas subluxation. Make no mistake for this is exactly what happens. The ramifications of the subluxation can extend to all parts of your body. In the most benign of these subluxations you may only experience a little lower back pain and in the more serious your whole body can be racked with pain and dysfunction. The tight sub-occipital ligaments and cervical spine muscles can be responsible for headaches or migraines as well as neck pain.
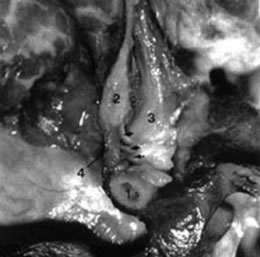 Figure 8: Myodural Bridge
Figure 8: Myodural Bridge Some years back Gary Hack D.D.S. et al 1995. "Anatomic relation between the rectus capitus posterior minor and the dura mater" Spine 20 (23): 2484-2486 discovers a previously unknown ligament directly attaching the posterior arch of the atlas to the dura mater of the brainstem and cerebellum. This attachment has become known as the myodural bridge and it is shown following in Figure 8.
The structures numbered in this dissection are as follows; 1. Posterior arch of the atlas; 2. Posterior occipital bone; 3. Rectus capitus posterior minor (RCPMI); 4; Dura mater of brainstem and cerebellum. The arrows indicate the myodural bridge attaching the posterior arch of the atlas to the dura mater of the brainstem & cerebellum. It is not difficult to see that any misalignment of the atlas with respect to the skull could traction the dura mater of the brainstem and cerebellum area. What would be the effects of such traction? Certainly it is possible for headaches and migraines to be an effect, but also there may well be other consequences. Researchers at Michigan State University; "College of Osteopathic Medicine" suggest "that the function of the RCPMI muscle is to provide static and dynamic proprioceptive feedback to the CNS (central nervous system), monitoring movement of the head and influencing movement of the surrounding musculature." In fact amongst other joints, the joints of the upper cervical spine are rich in proprioceptors, which provide positional feedback to the brain, in order for the brain to understand where the joints and therefore the head are in space and to make appropriate adjustments during movement. Close your eyes and point your first fingers on both hands. Now try and touch the tips of these fingers without opening your eyes. Your ability to touch your fingertips is an indication of your proprio receptive abilities. Any problems in this area may well be responsible for over and under corrections made by your brain, which would manifest as dizziness or balance disorders. Atlas subluxations, especially because they go hand in hand with some atrophy of these sub-occipital cervical muscles, could manifest as dizziness and/or balance disorders. Meniere's Disease has been associated with cervical dysfunction in a number of medical papers, and I have personally witnessed and know of other people diagnosed with Meniere's Disease who have had dramatic reversal of the disease's symptoms following upper cervical correction to their atlas vertebra by specific upper cervical chiropractors. This deserves further investigation as Meniere's Disease and other balance disorders are highly distressing to sufferers.
Now looking at Figure 7 further you will note that because the skull is tilted the pelvis will pull up on one side to compensate for the body imbalance and pull that leg off the ground. This is known as a functional short leg as opposed to an anatomical short leg. Of course, the leg is not off the ground because the weight of the body keeps it on the ground during walking. With the pelvis pulling up on one side the spinal column will now twist into scoliosis. Now the back muscles are contracting on one side which creates trigger points mainly at the 's' bend points in the scoliosis, lower back pain is evident and now hip problems can be a result. Leave this for long enough and the result may be surgical replacement of a degenerated hip. Knee, ankle, groin and calf problems can be a direct result, which people normally pass off as an aging thing or an accident. For me this explains the back pain all the way down my back and my ankle and knee problems, which corrected following correction of my atlas subluxation. The brain is the key initiator of this lifting of the pelvis, in order to align the pelvis and skeleton underneath the skull. There are cases of scoliosis that have resolved completely or at least improved considerably following upper cervical specific chiropractic correction of an atlas subluxation. Re-position the skull on top of the atlas, and thus cervical spine and the pelvis will be realigned directly underneath the skull.
Figures 9 & 10: NUCCA Types
Figures 9 & 10 reprinted with permission of National Upper Cervical Chiropractic Association - see Website www.nucca.org with special thanks to Robert Goodman, D.C. NUCCA
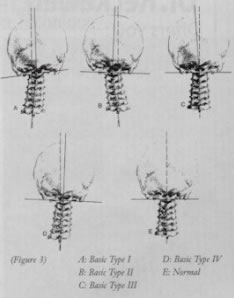 Figure 9 | 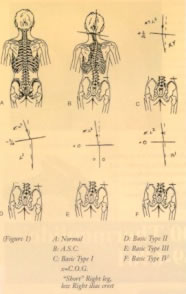 Figure 10 |
These graphics from the NUCCA site also show further the types of subluxations that can occur at the upper cervical spine level.
Which one actually occurs in each individual really depends upon their prevailing anatomy at that level and the direction and amplitude of the force imparted during the trauma they received. While it is not always the case, I have noticed that some people who have particularly large misalignments in their upper cervical spine sometimes can exhibit only minor symptoms, whilst others who have less of a misalignment can be in a very bad state in terms of the symptoms they are experiencing.
UPPER CERVICAL ANIMATIONS
The Sid E. William Research Center at Life University has some absolutely fantastic cervical spine animations showing different motions and subluxations within the cervical spine. I have chosen a couple of the animations to help explain further the anatomy of the atlas subluxation and what happens to the occipito-atlantal joint when there is a traumatic event. These animations follow herein.
The Sid E. William Research Center at Life University has some absolutely fantastic cervical spine animations showing different motions and subluxations within the cervical spine. I have chosen a couple of the animations to help explain further the anatomy of the atlas subluxation and what happens to the occipito-atlantal joint when there is a traumatic event. These animations follow herein.
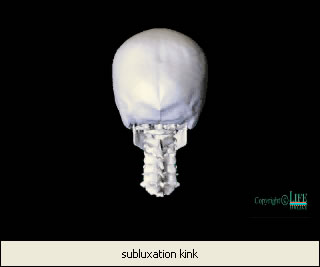 ANIMATION 1: The Kink Subluxation
ANIMATION 1: The Kink SubluxationAnimation 1: Copyright permission granted by Life University with special thanks to J. Roger Hinson, D.C.
This is known as the Grostic Kink Subluxation. This animation shows the movement of the skull and atlas with respect to the lower cervical spine.
To play the animation RIGHT CLICK the PICTURE and click Linked Video Clip Object and click Play Link or click on the following Hyperlink Kink Subluxation.
Within the Media Player you can use the slider to move the animation slowly through the subluxation. When you do this and leave the slider in a position about halfway along you will now note the position that the skull will be left in following a traumatic force to the skull, which stretches the ligaments strapping the skull to the upper cervical spine.
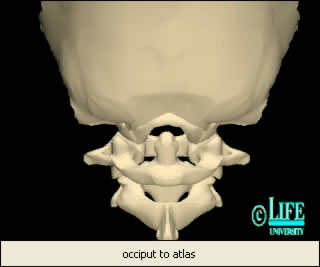 ANIMATION 2: The Occipito-Atlantal
ANIMATION 2: The Occipito-Atlantal Animation 2: Copyright permission granted by Life University with special thanks to J. Roger Hinson, D.C.
This animation shows the movement of the skull with respect to the atlas in lateral flexion to opposite sides. The skull slides with respect to the lower cervical spine, and because of the skull weight and ligaments its movement will drive and jam the atlas.
To play the animation RIGHT CLICK the PICTURE and click Linked Video Clip Object and click Play Link or click on the following Hyperlink Occiput to Atlas Subluxation.
Within the Media Player you can use the slider to move the animation slowly through the subluxation. When you do this and leave the slider in a position about halfway along you will now note the position that the skull will be left in following a traumatic force to the skull, which stretches the ligaments strapping the skull to the upper cervical
No comments:
Post a Comment