MS Lesions of the Cervical Cord
 and T2 weighted (d) Bra...")
Image via Wikipedia
Multiple Sclerosis is technically a neurodegenerative disease of the brain. Classically MS is associated with two or more supratentorial (above the covering over the cerebellum) periventricular hyperintensity signals. The lesions are the white spots on the brain scan on the right. The large shadows in the middle of the brain shaped like a butterfly are the lateral ventricles. The periventricular area surrounds the ventricles. In addition to the brain, however, some MS patients also get lesions in the cervical cord.
Demyelinating type lesions in the cervical cord without lesions in the brain are not considered to be classic signs of MS. Lesions below the cervical cord are, likewise, not considered to be MS. Instead they are given different names.In this post I will stick to MS lesions in the cervical cord and disregard lesions of the lower cord such as those seen in amyotrophic lateral sclerosis (ALS), primary lateral sclerosis, Devic’s Disease (neuromyelitis optica) and others. I will also ignore the lesions sometimes associated scoliosis and abnormal curvatures of the spine.
 According to Schelling, the lesions seen in the cervical cord in MS are due to stretch and shear stress. Many types of trauma, such as whiplash in the picture on the left, cause hyperflexion and hyperextension of the spine. The strain can occur in a front to back motion or from side to side. At the same time, whiplash type traumas also strain the spinal cord inside the spinal canal.
According to Schelling, the lesions seen in the cervical cord in MS are due to stretch and shear stress. Many types of trauma, such as whiplash in the picture on the left, cause hyperflexion and hyperextension of the spine. The strain can occur in a front to back motion or from side to side. At the same time, whiplash type traumas also strain the spinal cord inside the spinal canal. 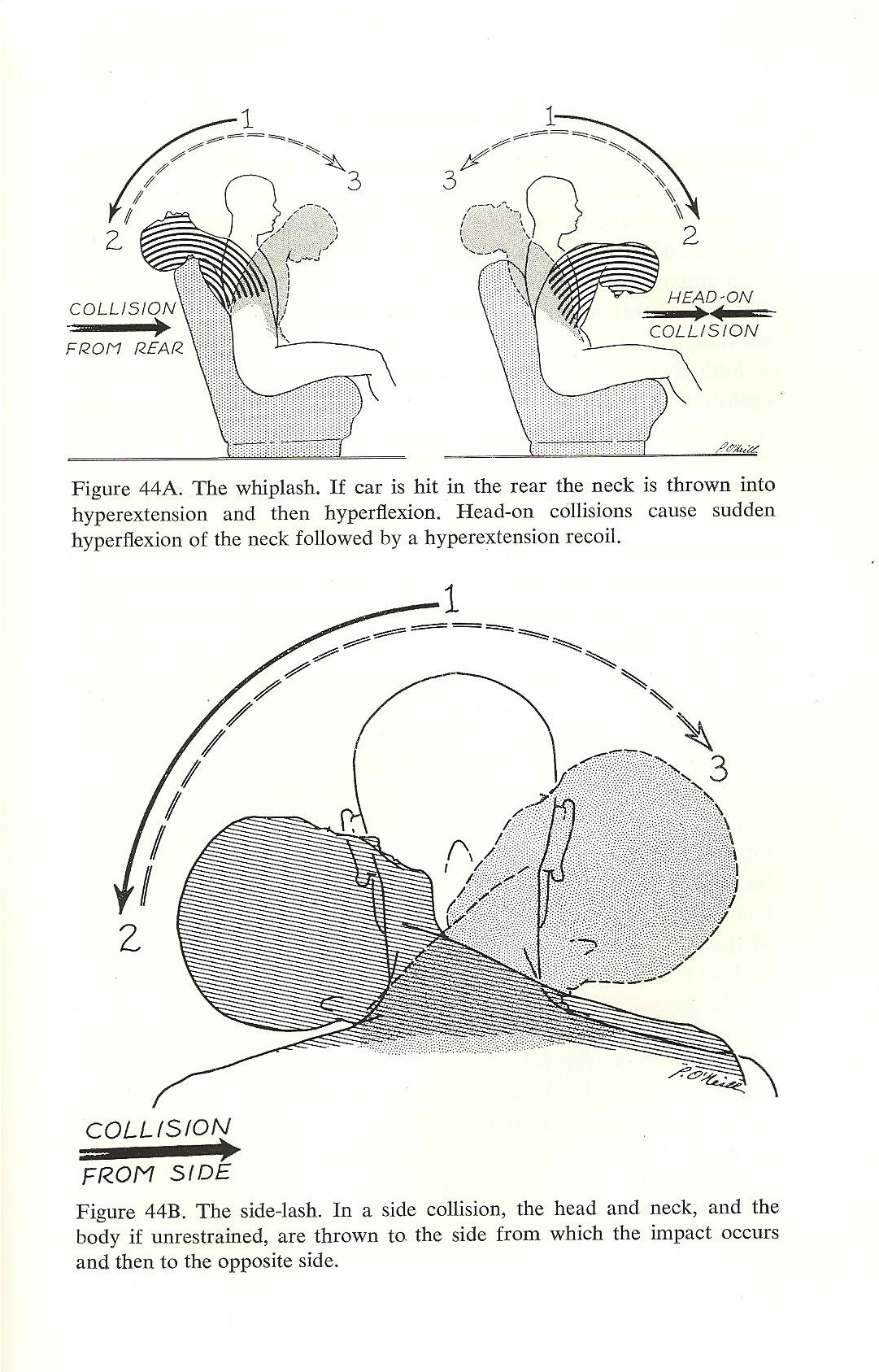{kind=link}
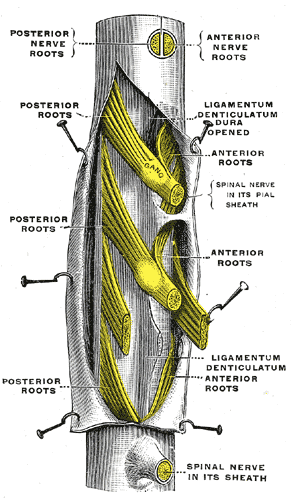
The spinal cord, like the brain has three protective coats called meninges. The outer coat is called the dura mater. The middle coat is called the subarachnoid mater and the inner coat is called the pia mater. Except for the attachment of the tail end of the cord, called the filum terminale, to the tail bone, called the coccyx, the spinal cord moves freely, unattached inside the spinal canal.

{kind=link}
{kind=link}
The three coats are held together by denticulate ligaments that attach the inner pia mater to the outer dura mater at the nerve roots. Click on the image on the right for a closer look. The subarchnoid space lies between the subarchnoid mater and the pia mater and contains a significant volume of cerebrospinal fluid, called CSF. There is also lymph like fluid that serves as a lubricant between the outer coat of the dura mater and the middle coat of the subarachnoid mater. This allows the inner contents of the cord to move somewhat independently to a limited degree.
 According to Schelling, mechanical strains of the spine can take the cord to extreme limits of stretch. It can also cause shear stress within the cord between the pia mater on the inside and the dura mater on the outside. The stress points occur at the attachment of the denticulate ligament. Furthermore, violent back jets of CSF in the subarachnoid space amplify the strain like a boat moored to a dock hit by hurricane force waves. The waves amplify the strain and rip the ropes and boats from their moorings. Similarly, violent waves of CSF flowing through the subarachnoid space amplify the strain acting on the denticulate ligaments. When they reach a critical threshold, engineer’s call the yeild point, the denticulate connective tissue attachments of the pia mater to the dura mater will tear. The strained tissues of the pia mater further damage the meylinated nerve tracts they cover. Click on the image above to get a closer look. This is a cross section of the cord and shows the inside. The H shape in the middle of the cord is the grey matter. The myelinated white fiber tracts surround it. The blue area is the subarachnoid space which contains CSF.
According to Schelling, mechanical strains of the spine can take the cord to extreme limits of stretch. It can also cause shear stress within the cord between the pia mater on the inside and the dura mater on the outside. The stress points occur at the attachment of the denticulate ligament. Furthermore, violent back jets of CSF in the subarachnoid space amplify the strain like a boat moored to a dock hit by hurricane force waves. The waves amplify the strain and rip the ropes and boats from their moorings. Similarly, violent waves of CSF flowing through the subarachnoid space amplify the strain acting on the denticulate ligaments. When they reach a critical threshold, engineer’s call the yeild point, the denticulate connective tissue attachments of the pia mater to the dura mater will tear. The strained tissues of the pia mater further damage the meylinated nerve tracts they cover. Click on the image above to get a closer look. This is a cross section of the cord and shows the inside. The H shape in the middle of the cord is the grey matter. The myelinated white fiber tracts surround it. The blue area is the subarachnoid space which contains CSF.
The lesions seen in the cervical cord are micro tears in the meninges and nearby myelinated nerve pathways . The tears cause scars to form called sclerotic plaques. Because they occur on the outside along the flanks of the cord, the tears tend to effect the outside structures of the cord.
The outside of the cord (see picture to left)contains the long myelinated high speed primary nerve pathways of the central nervous system. Primary nerves go from the brain to particular destination levels in the cord. The long white tracts on the outside of the cord contain both sensory nerves for detecting sensations related to the environment, muscle tone and balance, and motor nerves for running the muscles. Tears in the area of the denticulate ligaments thus affect nearby myelinated nerves in the cord resulting in muscle weakness and warped sensations called paresthesias.
In brief, according to Schelling, one of the likely causes of the lesions of multiple sclerosis seen in the brain are due to violent venous back jets associated with trauma. The lesions seen in the cervical cord are due to severe overstretching and shear stresses within the cord itself magnified by hydraulic stress from CSF waves. There is still more to the story, however, that needs further exploration and explanation. That’s where my theory may help to fill in some of the missing pieces to the puzzle.
My theory is that craniocervical syndromes can cause chronic edema (swelling), ischemia (decreased blood flow) and NPH (normal pressure hydrocephalus) conditions in the brain. Similar events can occur in the cord due to abnormal conditions of the spine. These chronic conditions can, in turn initiate neurodegenerative processes such as the glutamate cascade, which follows strokes.
In my next post I will discuss the posterior blood supply routes to the brain and circulation to the cord. The veins are not the only problem in MS. The arteries are a big part of the problem as well. In addition to MS, I suspect that certain cases of sclerosis of the long myelin tracts of the lower cord, such as ALS and PLS are probably due more to chronic ischemia. This is probably why lesions sometimes also show up in cases of abnormal curvatures of the spine such as scoliosis and kyphosis. Oxidative stress and chronic ischemia are chief suspects in the cause of demyelination and the shape of the spine, and thus the spinal canal, affect arterial and venous blood flow in the cord.
For additional information on this and related topics visit my website at http://www.upright-health.com.
No comments:
Post a Comment