snapping patients distal phalanx of middle finger leads to spontaneous flexion of other fingers
sustained clonus
> three beats defined as sustained clonus
sustained clonus has poor sensitivity (~13%) but high specificity (~100%) for cervical myelopathy
Babinski test
considered positive with extension of great toe
gait and balance
toe-to-heel walk
patient has difficulty performing
Romberg test
patient stands with arms held forward and eyes closed
loss of balance consistent with posterior column dysfunction
provocative tests
Lhermitte Sign
test is positive when extreme cervical flexion leads to electric shock-like sensations that radiate down the spine and into the extremities
Evaluation
Radiographs
recommended views
cervical AP, lateral, oblique, flexion, and extension views
general findings
degenerative changes of uncovertebral and facet joints
osteophyte formation
disc space narrowing
decreased sagittal diameter
cord compression occurs with canal diameter is < 13mm
lateral radiograph
important to look for diameter of spinal canal
a Pavlov ratio of less than 0.8 suggest a congenitally narrow spinal canal predisposing to stenosis and cord compression
sagittal alignment
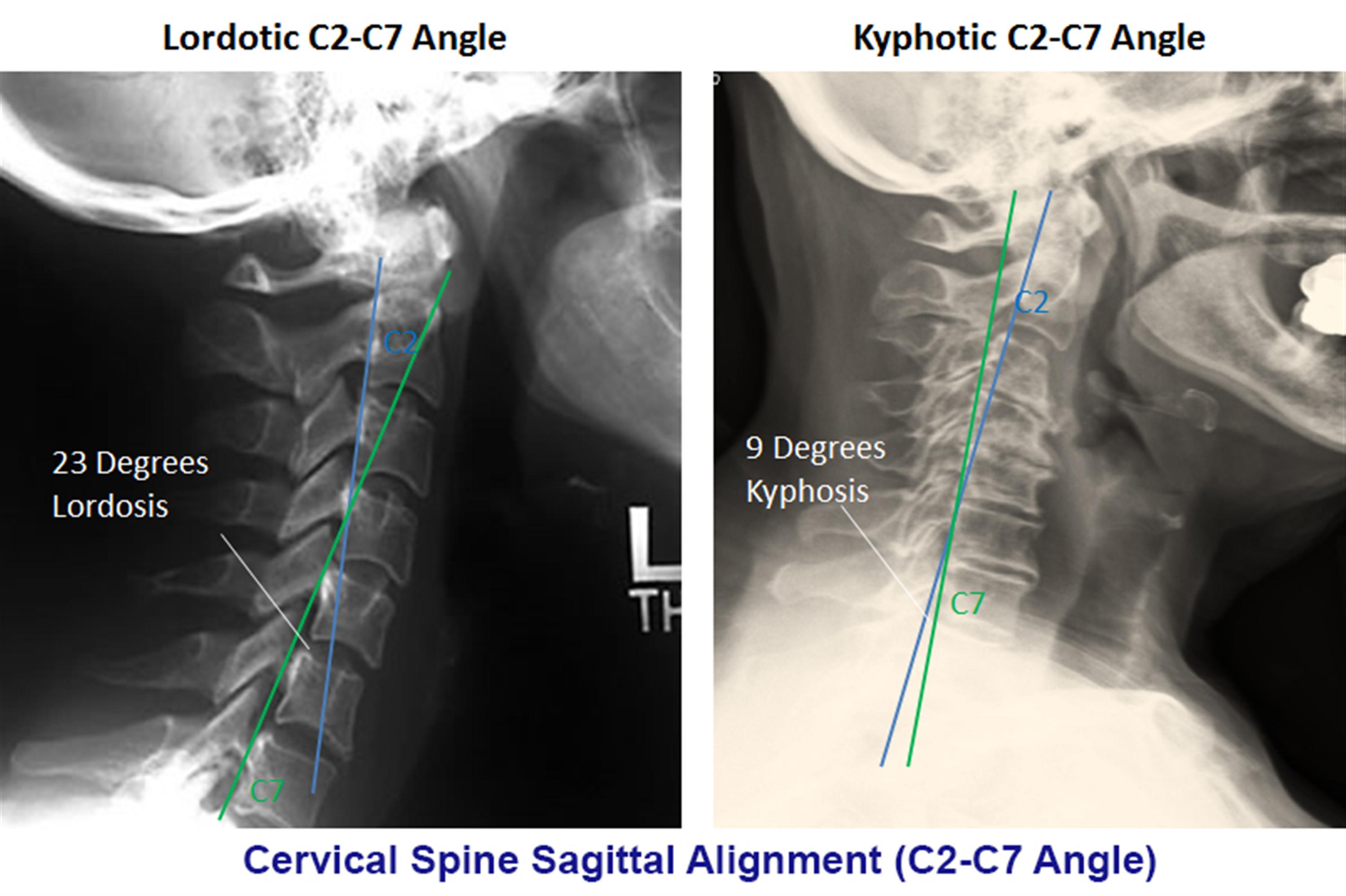
C2 to C7 alignment
determined by tangential lines on the posterior edge of the C2 and C7 body on lateral radiographs in neutral position
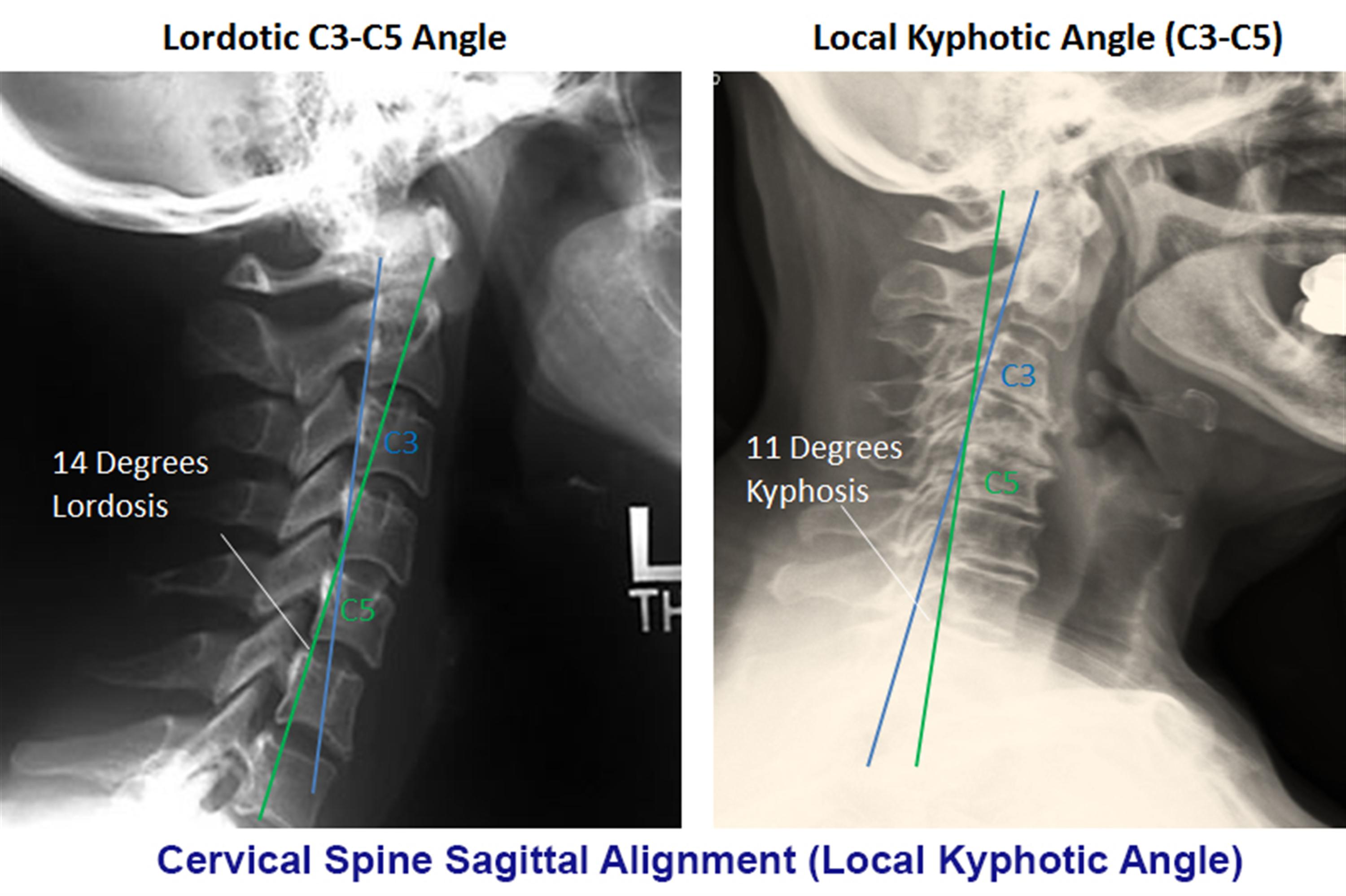
local kyphosis angle
the angle between the lines drawn at the posterior margin of most cranial and caudal vertebral bodies forming the maximum local kyphosis
oblique radiograph
important to look for foraminal stenosis which often caused by uncovertebral joint arthrosis
flexion and extension views
important to look for angular or translational instability
look for compensatory subluxation above or below the spondylotic/stiff segment
sensitivity/specificity
changes often do not correlate with symptoms
70% of patients by 70 yrs of age will have degenerative changes seen on plain xrays
MRI
indications
MRI is study of choice to evaluate degree of spinal cord and nerve root compression
findings
effacement of CSF indicates functional stenosis
spinal cord signal changes
seen as bright signal on T2 images (myelomalacia)
signal changes on T1-weighted images correlate with a poorer prognosis following surgical decompression
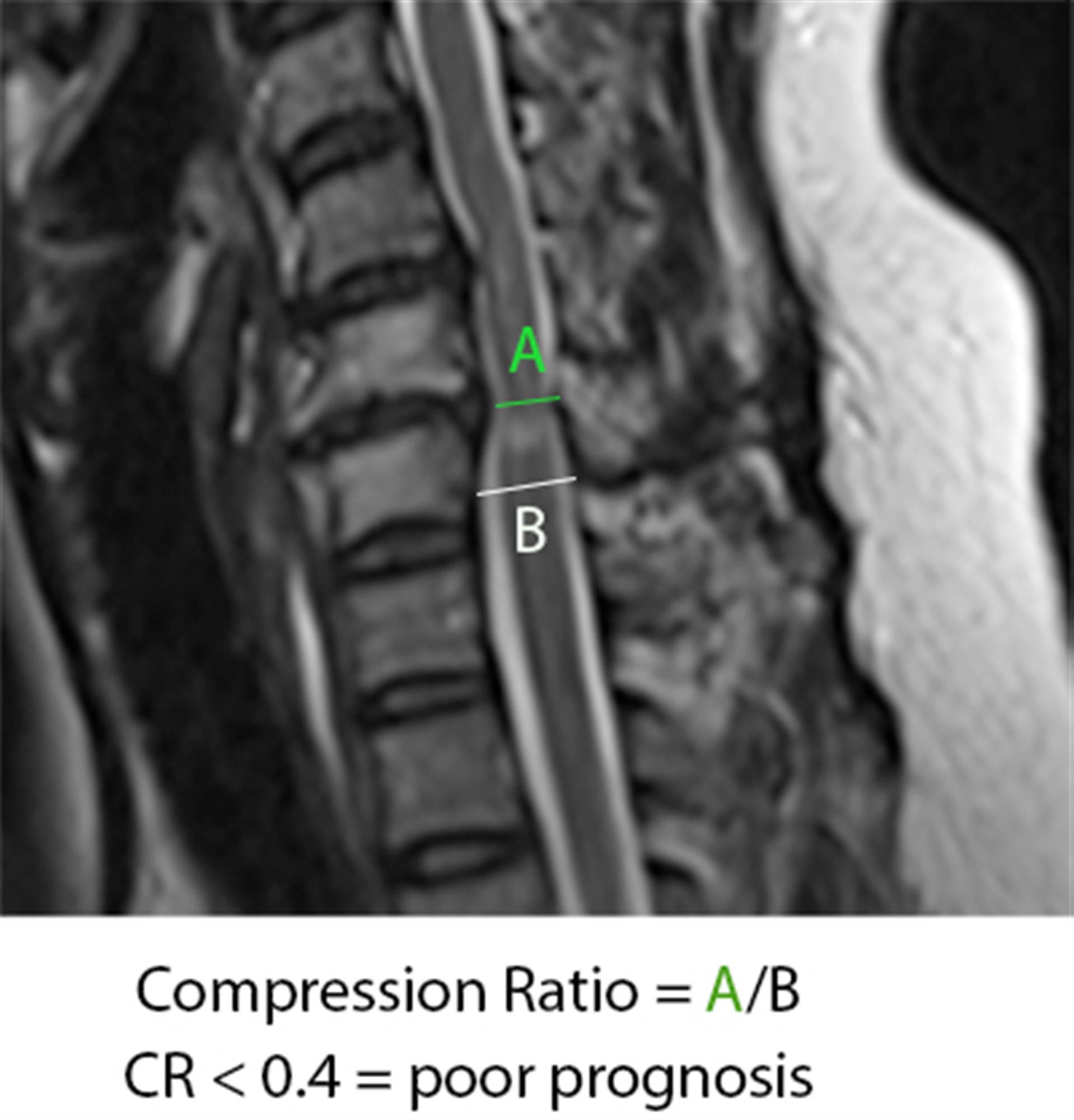
compression ratio of < 0.4 carries poor prognosis
CR = smallest AP diameter of cord / largest transverse diameter of cord
sensitivity/specificity
has high rate of false positive (28% greater than 40 will have findings of HNP or foraminal stenosis)
CT without contrast
can provide complementary information with an MRI, and is more useful to evaluate OPLL and osteophytes
CT myelography
more invasive than an MRI but gives excellent information regarding degrees of spinal cord compression
useful in patients that cannot have an MRI (pacemaker), or have artifact (local hardware)
contrast given via C1-C2 puncture and allowed to diffuse caudally, or given via a lumbar puncture and allowed to diffuse proximally by putting patient in trendelenburg position.
Nerve conduction studies
high false negative rate
may be useful to distinguish peripheral from central process (ALS)
Differential
Normal aging
mild symptoms of myelopathy often confused with a "normal aging" process
Stroke
Movement disorders
Vitamin B12 deficiency
Amyotrophic lateral sclerosis (ALS)
Multiple sclerosis
Treatment
Nonoperative
observation, NSAIDs, therapy, and lifestyle modifications
indications
mild disease with no functional impairment
function is a more important determinant for surgery than physical exam finding
patients who are poor candidates for surgery
modalities
medications (NSAIDS, gabapentin)
immobilization (hard collar in slight flexion)
physical therapy for neck strengthening, balance, and gait training
traction and chiropractic modalities are not likely to benefit and do have some risks
be sure to watch patients carefully for progression
outcomes
improved nonoperative outcomes associated with patients with larger transverse area of the spinal cord (>70mm2)
some studies have shown improvement with immobilization in patients with very mild symptoms
Operative
surgical decompression, restoration of lordosis, stabilization
indications
significant functional impairment AND
1-2 level disease
lordotic, neutral or kyphotic alignment
techniques
appropriate procedure depends on
cervical alignment
number of stenotic levels
location of compression
medical conditions (e.g., goiter)
treatment procedures include (see below)
anterior cervical diskectomy/corpectomy and fusion
posterior laminectomy and fusion
posterior laminoplasty
combined anterior and posterior procedure
cervical disk arthroplasty
outcomes
prospective studies show improvement in overall pain, function, and neurologic symptoms with operative treatment
early recognition and treatment prior to spinal cord damage is critical for good clinical outcomes
Techniques
Goals
optimal surgical treatment depends on the individual. Things to consider include
number of stenotic levels
sagittal alignment of the spine
degree of existing motion and desire to maintain
medical comorbidities (eg, dysphasia)
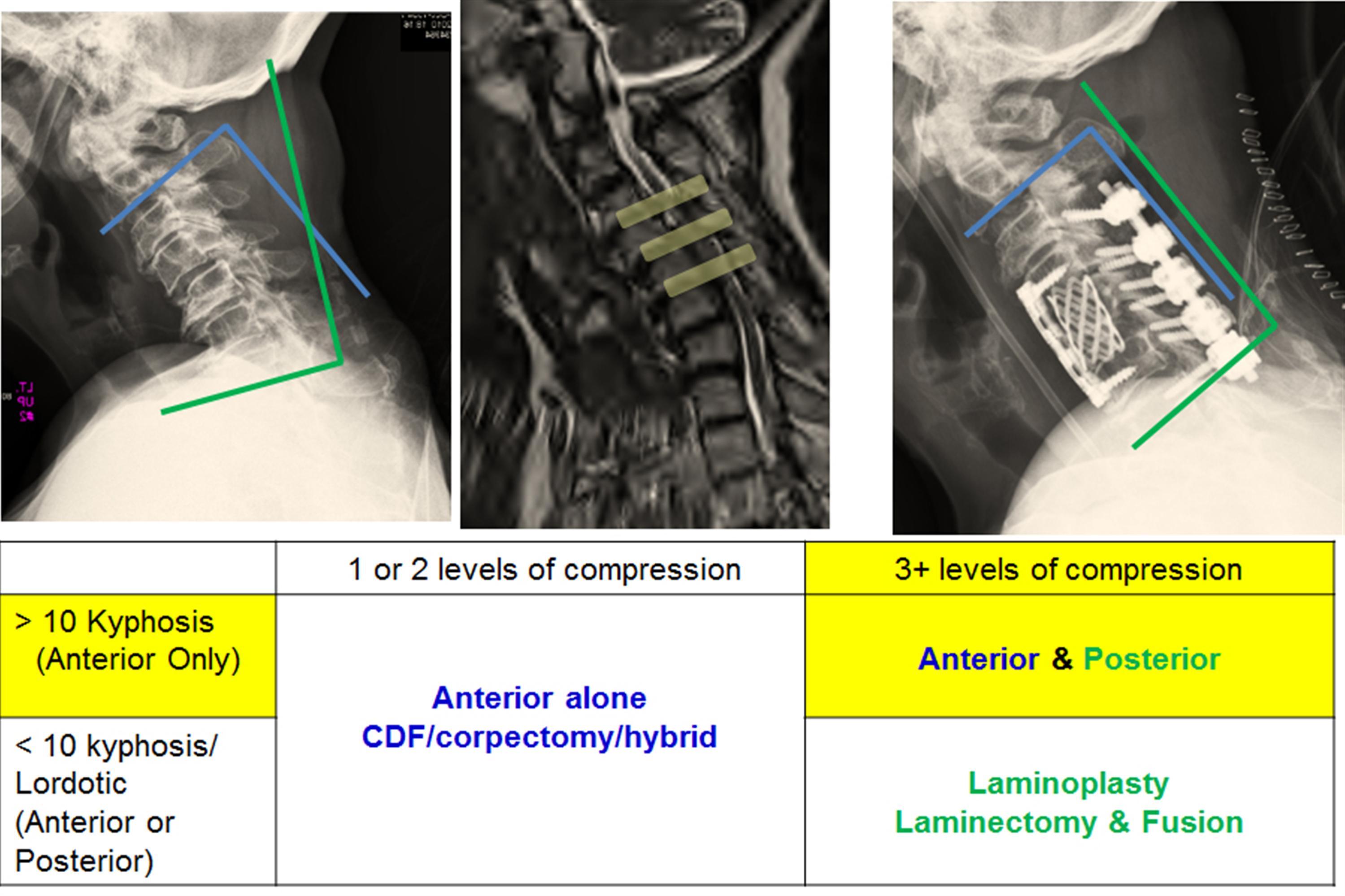
simplified treatment algorithm
Anterior Decompression and Fusion (ACDF) alone
indications
mainstay of treatment in most patients with single or two level disease
fixed cervical kyphosis of > 10 degrees
anterior procedure can correct kyphosis
compression arising from 2 or fewer disc segments
pathology is anterior (OPLL, soft discs, disc osteophyte complexes)
approach
uses Smith-Robinson anterior approach
decompression
corpectomy and strut graft may be required for multilevel spondylosis
two level corpectomies tend to be biomechanically vulnerable (preferable to combine single level corpectomy with adjacent level diskectomy)
7% to 20% rates of graft dislodgement with cervical corpectomy with associated severe complications, including death, reported.
fixation
anterior plating functions to increase fusion rates and preserve position of interbody cage or strut graft
pros & cons
advantages
lower infection rate
mild postoperative pain
complications & disadvantages
avoid in patients with poor swallowing function
Laminectomy with posterior fusion
indications
multilevel compression with kyphosis of < 10 degrees
> 13 degrees of fixed kyphosis is a contraindication for a posterior procedure
in flexible kyphotic spine, posterior decompression and fusion may be indicated if kyphotic deformity can be corrected prior to instrumentation
contraindications
fixed kyphosis of > 10 degrees is a contraindication to posterior decompression
will not adequately decompress spinal cord as it is "bowstringing" anterior
pros & cons
fusion may improve neck pain associated with degenerative facets
not effective in patients with > 10 degrees fixed kyphosis
Laminoplasty
indications
gaining in popularity
useful when maintaining motion is desired
avoids complications of fusion so may be indicated in patients at high risk of pseudoarthrosis
contraindications
cervical kyphosis
> 13 degrees is a contraindication to posterior decompression
will not adequately decompress spinal cord as it is "bowstringing" anterior
severe axial neck pain
is a relative contraindication and these patients should be fused
technique
volume of canal is expanded by hinged-door laminoplasty followed by fusion
usually performed from C3 to C7
open door technique
hinge created unilateral at junction of lateral mass and lamina and opening on opposite side
opening held open by bone, suture anchors, or special plates
French door technique
hinge created bilaterally and opening created midline
pros & cons
advantages
allows for decompression of multilevel stenotic myelopathy without compromising stability and motion (avoids postlaminectomy kyphosis)
lower complication rate than multilevel anterior decompression
especially in patients with OPLL
a motion-preserving technique
pseudoarthrosis not a concern in patients with poor healing potential (diabetes, chronic steroid users)
can be combined with a subsequent anterior procedure
disadvantage
postoperative neck pain
still associated with loss of motion
outcomes
equivalent to multilevel anterior decompression and fusion
Combined anterior and posterior surgery
indications
multilevel stenosis in the rigid kyphotic spine
multi-level anterior cervical corpectomies
postlaminectomy kyphosis
Laminectomy alone
indications
rarely indicated due to risk of post laminectomy kyphosis
pros & cons
progressive kyphosis
11 to 47% incidence if laminectomy performed alone without fusion
Complications
Pseudoarthrosis
incidence
12% for single level fusions, 30% for multilevel fusions
treatment
treat with either posterior wiring or plating or repeat anterior decompression and plating if patient has symptoms of radiculopathy
Postoperative C5 palsy
incidence
reported to occur in ~ 4.6% of patients after surgery for cervical compression myelopathy
no significant differences between patients undergoing anterior decompression and fusion and posterior laminoplasty
occurs immediately postop to weeks following surgery
mechanism
mechanism is controversial
in laminectomy patients, it is thought to be caused by tethering of nerve root with dorsal migration of spinal cord following removal of posterior elements
prognosis
patients with postoperative C5 palsy generally have a good prognosis for functional recovery, but recovery takes time
Recurrent laryngeal nerve injury
approach
in the past it has been postulated that the RLN is more vulnerable to injury on the right due to a more aberrant pathway
recent studies have shown there is not an increased injury rate with a right sided approach
treatment
if you have a postoperative RLN palsy, watch over time
if not improved over 6 weeks than ENT consult to scope patient and inject teflon
if you are performing revision anterior cervical surgery, and there is an any suspicion of a RLN from the first operation, obtain ENT consult to establish prior injury
if patient has prior RLN nerve perform revision surgery on the same as the prior injury/approach to prevent a bilateral RLN injury
Hardware failure and migration
7-20% with two level anterior corpectomies
two level corpectomies should be stabilized from behind
(SBQ12.5) A 70-year-old presents with gait instability and difficulty buttoning his shirts which has been progressively worsening over the last several months. His physical exam is notable for exaggerated patellar reflexes and sustained clonus. The provocative maneuver shown in Figure V would most likely produce which of the following symptoms or physical exam finding? Review Topic
The video shown in Figure V shows a Lhermitte maneuver which is a provocative maneuver used in the diagnosis of cervical myelopathy. When it is positive the patient will complain of electric shock-like sensations that radiate down the spine and into the extremities.
The Lhermitte sign was originally described in 1917 to describe the “pins and needles” sensations that passed through the extremities when the neck is flexed. The test is highly specific, but not sensitive, for cervical spinal cord compression or myelopathy. It may be positive in multiple conditions, including multiple sclerosis.
Uchihara et al. studied the relationship between pain with compression of the brachial plexus (BP) and cervical spine pathology. They found pain with compression of the brachial plexus (BP) was quite sensitive and reasonably specific to detect compressive neuropathies of the cervical spine.
Rhee et al. looked at the sensitivity and specificity of different physical exam findings for cervical myelopathy. They found sustained clonus was poorly sensitive (13%) but highly specific (100%) for cervical myelopathy. Given that 20% of myelopathic patients may not have typical exam findings (ie. clonus, Babinski, hyper-reflxia), they recommend that appropriate patient management be guided by individual history, physical exam and imaging findings.
Figure V demonstrates the Lhermitte provocative maneuver
Incorrect Answers: Answer 2: Involuntary thumb IP joint contraction is associated with a Hoffman’s pathologic reflex Answer 3: Spontaneous abduction of the 5th digit (finger escape sign) is associated with weak intrinsic muscles in the setting of cervical myelopathy Answer 4: Spontaneous extension of the great toe may be associated with a pathologic upper motor neuron reflex (i.e. Babinski sign) Answer 5: Unilateral arm pain and paresthesias in a dermatomal distribution is consistent with cervical radiculopathy and may be elicited with the Spurling test.
REFERENCES:
1. Rhee JM, Heflin JA, Hamasaki T, Freedman B. Prevalence of physical signs in cervical myelopathy: a prospective, controlled study. Spine (Phila Pa 1976). 2009 Apr 20;34(9):890-5. doi: 10.1097/BRS.0b013e31819c944b. PubMed PMID: 19352222. PMID:19352222 (Link to Abstract)
2. Uchihara T, Furukawa T, Tsukagoshi H. Compression of brachial plexus as a diagnostic test of cervical cord lesion. Spine (Phila PA 1976). 1994 Oct 1;19(19):2170-3 PMID:7809749 (Link to Abstract)
(SBQ12.16) A 50-year-old female presents with 3 years of increasing clumsiness in her hands that has progressed to the point that it is now difficult to open jars and use her keys. On physical exam she is unable to perform a tandem gait, has positive Hoffman’s signs bilaterally, and has 3+ patellar reflexes. She has 5/5 strength in all her major muscle groups. Figure A is her mid sagittal MRI. Figure B, C and D are axial images at C4/5, C5/6 and C6/7 respectively. What is the most appropriate treatment? Review Topic
The patient has signs and symptoms of progressive cervical myelopathy with CSF effacement and cord compression at C5/6 and C6/7. At this point, the most appropriate treatment is a 2-level ACDF
Classically patients with cervical myelopathy present with a stepwise progression of worsening symptoms. Patients often complain of balance issues, numbness and weakness in their hands, and difficulty with fine motor tasks. Patients with progressive myelopathy and significant functional impairment should undergo surgery to decompress the spinal cord.
Emery et al. reported on 108 patients who underwent an anterior cervical decompression and fusion for the treatment of cervical myelopathy. Almost all patients had some neurologic improvement, and the strongest predictor of the amount of improvement was the severity of symptoms prior to surgery. Recurrent myelopathy was rare, and only occurred in cases of pseudarthrosis or stenosis at a new level.
Komotar et al. discussed the role for posterior surgery for cervical myelopathy, and he concluded that a posterior laminectomy and fusion is preferable for patients with a lordotic cervical spine and either three or more levels of compression, primarily posterior compression or diffuses congenital stenosis.
Figures A-D demonstrate compression of the spinal cord at C5/6 and C6/7.
Incorrect Answers: Answer 1: The patient has progressive myelopathy, observation is not appropriate. Answer 2: The patient has progressive myelopathy, neither observation nor an ESI are appropriate. Answer 4: A posterior cervical laminectomy without fusion can lead to post-laminectomy kyphosis. Answer 5: A foraminotomy will not decompress the spinal cord.
REFERENCES:
1. Emery SE, Bohlman HH, Bolesta MJ, Jones PK. Anterior cervical decompression and arthrodesis for the treatment of cervical spondylotic myelopathy. Two to seventeen-year follow-up. J Bone Joint Surg Am. 1998;80(7):941-951. PMID:9697998 (Link to Abstract)
2. Komotar RJ, Mocco J, Kaiser MG. Surgical management of cervical myelopathy: indications and techniques for laminectomy and fusion. Spine J. 2006;6(6 Suppl):252S-267S. PMID:17097545 (Link to Abstract)
(SBQ09.3) Figures A-E show the neutral lateral cervical radiographs and corresponding T2-weighted MRI of 5 patients with symptoms and physical exam findings consistent with cervical myelopathy. In which of these patients would a cervical laminoplasty alone be contraindicated as surgical treatment? Review Topic
Laminoplasty alone as surgical treatment is contradindicated in patients with rigid cervical kyphosis of > 13 degrees as shown in Figure D.
When evaluating patients with cervical myelopathy, it is critical to evaluate the sagittal alignment of the cervical spine. This is best done on lateral cervical spine films in neutral, flexion, and extension. By obtaining flexion and extension films, one can determine if the kyphotic deformity is rigid or not. Two angles should be measured, the C2-7 kyphotic angle, and the local kyphotic angle. If patients have significant kyphosis, the spinal cord is draped over the anterior compressive elements, and a posterior approach alone, such as a laminoplasty, is not effective.
Suda et al. showed that local kyphosis was the most crucial risk factor for poor surgical outcomes with laminoplasty alone. They recommend when patients have local kyphosis exceeding 13 degrees, anterior decompression should be performed with an attempt to correct the deformity, followed by posterior decompression in some cases. Expansive laminoplasty alone should be avoided in patients with local kyphosis greater than 13 degrees.
Chiba et al. reviewed the long-term results of open-door laminoplasty for cervical myelopathy in patients with ossification of the posterior longitudinal ligament. They found patients with preoperative kyphosis had lower recovery rates than those with straight and lordotic alignments.
Illustration A and B show the methodology of how to measure the C2-C7 kyphotic angle and the local kyphosis angle. The C2-7 angle is determined by tangential lines on the posterior edge of the C2 and C7 body on lateral radiographs in neutral position. The local kyphosis angle is determined by tangential lines on the posterior edge of the vertebral bodies that flank the kyphotic segment. Illustration C shows the treatment algorithm of cervical myelopathy.
Incorrect Answers: Answer 1, 2, 3, 5: The mainstay of treatment in most patients with multi-level disease would be laminectomy with posterior fusion (if kyphosis is <10 degree) or a combined anterior and posterior approach (if kyphosis is >10 degrees).
1. Suda K, Abumi K, Ito M, Shono Y, Kaneda K, Fujiya M. Local kyphosis reduces surgical outcomes of expansive open-door laminoplasty for cervical spondylotic myelopathy. Spine (Phila Pa 1976). 2003 Jun 15;28(12):1258-62. PubMed PMID: 12811268. PMID:12811268 (Link to Abstract)
2. Chiba K, Ogawa Y, Ishii K, Takaishi H, Nakamura M, Maruiwa H, Matsumoto M, Toyama Y. Long-term results of expansive open-door laminoplasty for cervical myelopathy--average 14-year follow-up study. Spine (Phila Pa 1976). 2006 Dec 15;31(26):2998-3005. PubMed PMID: 17172996. PMID:17172996 (Link to Abstract)
(OBQ12.174) A 47-year old female with Type-2 diabetes and a pacemaker presents with bilateral buttock and leg pain that is worse with prolonged walking and improves with sitting. Her lower extremity symptoms are severe enough that she reports she feels "unstable" on her feet. Physical exam shows 5/5 strength in all muscles groups in the lower extremity. Figure V shows a result of forced ankle dorsiflexion on physical exam. A lumbar myelogram is performed and shown in Figure A, B, and C. What is the most appropriate next step in treatment. Review Topic
The clinical presentation and imaging studies are consistent with concurrent symptoms of myelopathy and neurogenic claudication in a patient with lumbar degenerative spondylolisthesis. An CT myelogram of the cervical spine would be the most appropriate next step in management as the patient is unable to obtain an MRI due to the pacemaker.
Symptomatic tandem stenosis can present with a confusing scenario of both neurogenic claudication and myelopathy. The prevalence has been estimated to be from 5% to 25%. Depending on the severity of symptoms, the cervical myelopathy usually takes treatment precedence.
Lee et al. performed a cadaveric study looking at the incidence of tandem stenosis. They found a prevalence of tandem stenosis from 0.9% to 5.4% in the sample population. The association of cervical and lumbar stenosis was found to be statistically significant, and stenosis in one part of the spine positively predicts for stenosis in the other area of the spine 15.3% to 32.4% of the time.
Eskander et al. looked at the ideal treatment algorithm (staged or simultaneous) in patients with symptomatic tandem stenosis in the lumbar and cervical spine. They report treatment outcomes are similar regardless of the surgical choice, but that complications are significantly increased by increasing patient age, blood loss, and operative time. Therefore, the decision to approach the lumbar and cervical spine simultaneously or staged depends on the characteristic of the patient and whichever approach the surgeon feels will minimize blood loss and operative time.
Rhee et al. looked at the sensitivity and specificity of different physical exam findings for cervical myelopathy. They found sustained clonus was poorly sensitive (13%) but highly specific (100%) for cervical myelopathy.
Figure A, B, and C show a lumbar myelogram in AP, flexion, and extension respectively. There is a degenerative spondylolisthesis with associated spinal stenosis. Figure V is a video showing sustained clonus with forced ankle dorsiflexion. 3 beats of clonus or less is considered normal. Illustration A is a table from the Rhee study which shows the sensitivity and specificity of different physical exam findings for cervical myelopathy.
Incorrect Answers: Answer 1: The patient has degenerative spondylolisthesis, and therefore even after the cervical spine is evaluated, a laminectomy alone would not be indicated. Answer 2,3 and 4: All of these are appropriate treatment options for the degenerative spondylolisthesis in this patient. However the question asks for the next step in management, would should be focused evaluating the cervical spine.
1. Lee MJ, Garcia R, Cassinelli EH, Furey C, Riew KD. Tandem stenosis: a cadaveric study in osseous morphology. Spine J. 2008 Nov-Dec;8(6):1003-6. Epub 2008 Feb 14. PubMed PMID: 18280216 PMID:18280216 (Link to Abstract)
2. Eskander MS, Aubin ME, Drew JM, Eskander JP, Balsis SM, Eck J, Lapinsky AS, Connolly PJ. Is there a difference between simultaneous or staged decompressions for combined cervical and lumbar stenosis? J Spinal Disord Tech. 2011 Aug;24(6):409-13. PubMed PMID: 21150658. PMID:21150658 (Link to Abstract)
3. Rhee JM, Heflin JA, Hamasaki T, Freedman B. Prevalence of physical signs in cervical myelopathy: a prospective, controlled study. Spine (Phila Pa 1976). 2009 Apr 20;34(9):890-5. doi: 10.1097/BRS.0b013e31819c944b. PubMed PMID: 19352222. PMID:19352222 (Link to Abstract)
(OBQ12.247) A 51-year-old presents for evaluation of clumsiness of her hands. She complaints of difficulty with buttoning her shirt. On physical exam she is unable to preform a tandem gait. The strength in her upper extremities proximally is graded a 4/5, but she has significant bilateral intrinsic hand weakness and a positive Hoffmann's sign. When told to hold her fingers in an extended and adducted position, her ring and small fingers flex and abduct within 20 seconds. What is the most appropriate next step in management? Review Topic
1. Reassurance and period of observation
0% (3/1289)
2. Night splinting in cock-up wrist splints
0% (5/1289)
3. Carpal tunnel corticosteroid injection
0% (3/1289)
4. Electromyographic studies of the upper extremities
This patient’s clinical presentation is concerning for cervical myelopathy. The inability to preform a tandem gait, intrinsic wasting, a positive Hoffmann's sign, and a finger escape sign(the two ulnar digits drift into abduction and flexion within 30 seconds) are all signs of myelopathy. Obtaining a cervical spine MRI is necessary to confirm the diagnosis and initiate treatment.
Cervical myelopathy is a disease caused by compression of the spinal cord and is associated with a constellation of symptoms including difficulty with gait and clumsiness of the hands. It can be graded using the modified Japanese Orthopedic Association Scale. (Illustration A)
Emery et al. reviewed the natural history, pathogenesis, diagnosis and management of cervical spondylotic myelopathy. The natural history of cervical myelopathy is slow, stepwise deterioration over time, with variable periods of stable neurologic function. Surgical intervention is indicated to alter the natural history and prevent further progression.
Rao et al. discuss the pathophysiology, natural history, and clinical evaluation of cervical myelopathy. The clinical presentation of myelopathy is described as highly variable. Diffuse numbness in the hands is often misdiagnosed as carpal tunnel syndrome and requires a high index of suspicion given the progressive deterioration in patients with cervical myelopathy.
Rhee et al. compared the physical exam findings of 39 patients with myelopathy to 37 without, and while he found a significant increase in myelopathic signs on physical exam in the myelopathy group, 21% of patients in the myelopathy group had no myelopathic signs of physical exam. Individual tests were even less reliable, with a Hoffmann sign only present in 59%, Babinski in 13%, and clonus in 13%.
Illustration A is the modified Japanese Orthopedic Association Scale. Illustrations B and C show the sagittal and axial T2-weighted MRI sequences from the patient in this scenario. There is extensive cervical spondylosis and cord compression.
Incorrect Answers: Answer 1: Reassurance and observation is inappropriate in cervical myelopathy; the nature of this process is progressive deterioration Answer 2: Night splinting is an appropriate first line treatment in carpal tunnel syndrome, not cervical myelopathy Answer 3: Carpal tunnel corticosteroid injections are not appropriate treatment in patients with cervical myelopathy Answer 4: EMG studies may show evidence of cervical radiculopathy, but they are not the appropriate next step in this patient’s management
2. Emery SE. Cervical spondylotic myelopathy: diagnosis and treatment. J Am Acad Orthop Surg. 2001 Nov-Dec;9(6):376-88. Review. PubMed PMID: 11767723. PMID:11767723 (Link to Abstract)
3. Rao R. Neck pain, cervical radiculopathy, and cervical myelopathy: pathophysiology, natural history, and clinical evaluation. J Bone Joint Surg Am. 2002 Oct;84-A(10):1872-81. Review. PubMed PMID: 12377921. PMID:12377921 (Link to Abstract)
4. Rhee JM, Heflin JA, Hamasaki T, Freedman B. Prevalence of physical signs in cervical myelopathy: a prospective, controlled study. Spine (Phila Pa 1976). 2009;34(9):890-895. PMID:19352222 (Link to Abstract)
(OBQ11.209) A 56-year-old woman presents for initial evaluation of her neck pain which has been worsened by activity for the last several years. On exam, she has 5/5 motor strength throughout bilateral upper and lower extremities. She has a normal gait and no difficulties with manual dexterity. Reflex testing shows hyperreflexia in bilateral Achilles tendons. Lateral radiographs are shown in Figure A, and MRI scan is shown in Figures B and C. What is the most appropriate management? Review Topic
The patient's clinical picture is consistent with cervical spondylosis. Minimal symptoms without hard evidence of gait disturbance or pathologic reflexes warrant nonoperative treatment, making physical therapy the correct answer.
Cervical spondylosis is a process that results in disc degeneration and facet arthropathy. Clinical manifestations may range from axial neck pain to profound muscle weakness and difficulties ambulating. It is generally agreed upon that patients with neuroradiologic evidence of spinal cord compression but no signs of myelopathy should be managed non-operatively. Initial management should consist of physical therapy, NSAIDs, and a cervical collar for comfort.
Boden and McCowin et al. describe the prevalence of abnormal cervical spine MRI findings in asymptomatic patients. 19 percent of asymptomatic patients were found to have abnormal scans. The most common finding in subjects less than 40 years old was a herniated disc, while the most common finding in subjects greater than 40 years of age was foraminal stenosis.
Kadanka and Mares et al. provide a prospective, randomized study comparing conservative and operative treatment of mild and moderate forms of spondylotic cervical myelopathy. At the 3-year follow-up period, there were no significant differences between the surgical and conservative treatment groups.
Figure A shows a lateral radiograph with loss of cervical lordosis and mild degenerative changes at C5-6, C6-7. Figures B shows a sagittal MRI with mild stenosis and loss of cervical lordosis. Figure C shows the axial MRI with left-sided foraminal stenosis at C5-6.
Incorrect Answers: Answers 1-4: non-operative management is recommended in this situation.
REFERENCES:
1. Boden SD, McCowin PR, Davis DO, Dina TS, Mark AS, Wiesel S. Abnormal magnetic-resonance scans of the cervical spine in asymptomatic subjects. A prospective investigation. J Bone Joint Surg Am. 1990 Sep;72(8):1178-84. PMID:2398088 (Link to Abstract)
2. Kadanka Z, Mares M, Bednanik J, Smrcka V, Krbec M, Stejskal L, Chaloupka R, Surelova D, Novotny O, Urbanek I, Dusek L. Approaches to spondylotic cervical myelopathy: conservative versus surgical results in a 3-year follow-up study. Spine (Phila PA 1976). 2002 Oct 15;27(20):2205-10; discussion 2210-1. PMID:12394893 (Link to Abstract)
(OBQ11.251) A 68-year-old female presents with progressive loss of ability to ambulate and dexterity problems with her hands. Six months ago she was able to walk with a cane, but now has difficulty with ambulating with a walker. She also reports difficulty with her hands and needs assistance with eating. Physical exam shows limited neck extension. Radiographs, tomography, and magnetic-resonance-imaging are shown in Figure A, B, and C respectively. What is the most appropriate treatment? Review Topic
The patients symptoms are consistent with progressive cervical myelopathy. Her symptoms are progressive and severe, and therefore surgical decompression is indicated. She has cervical kyphosis as demonstrated on physical exam and imaging, with compression at three levels (C3/4, C4/5, C5/6). An anterior procedure is mandatory to correct her kyphosis and remove the anterior compressive lesions. Of the options listed, only answer 5 involves an anterior procedure, and therefore, it is the most appropriate treatment.
Possible treatment options in this case could: 1) multi-level ACDF with anterior plate fixation, 2) a hybrid C5 corpectomy with ACDF as C3/4 and anterior plate fixation, or 3) a C3 and C4 corpectomy, anterior plate fixation, followed by posterior decompression and fusion. It is important to remember any two level corpectomy needs to be stabilized posterior due to the high rate of graft migration.
Suda et al showed that signal intensity change on MRI and local kyphosis were the most crucial risk factors for poor surgical outcomes. They recommend when patients have local kyphosis exceeding 13 degrees, anterior decompression should be performed with an attempt to correct the deformity, followed by posterior decompression in some cases. Expansive laminoplasty alone should be avoided in patients with local kyphosis greater than 13 degrees.
Chiba et al reviewed the long-term results of open-door laminoplasty for cervical myelopathy. They found satisfactory results of open-door laminoplasty at an average follow up of 14 years. Overall cervical range of motion decreased by 36%. Segmental motor palsy developed in 8 of 80 patients.
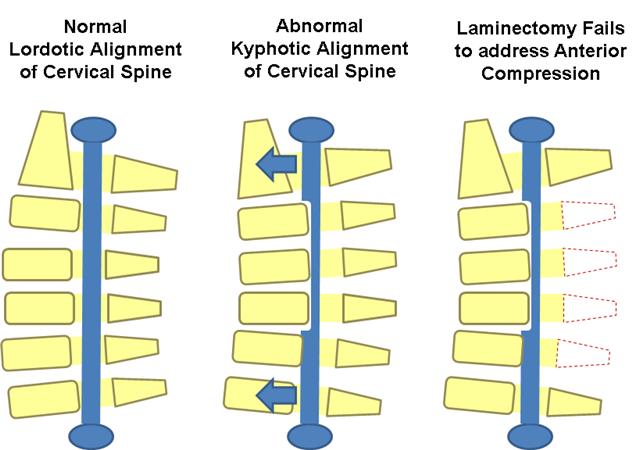
Illustration A demonstrates why a posterior decompression is ineffective in patients with rigid kyphosis and cervical myelopathy.
Incorrect Answers: Answer 1: Due to her severe and progressive symptoms, there is no role for nonoperative treatment in this patient. Answer 2, 3, 4: Any posterior procedure alone, including a laminectomy, laminectomy with fusion, or laminoplasty would not correct her kyphotic deformity and address the anterior compression caused by the spinal cord "draping" over the anterior compressive elements. A posterior procedure alone should be avoided in patients with excessive kyphosis.
1. Suda K, Abumi K, Ito M, Shono Y, Kaneda K, Fujiya M. Local kyphosis reduces surgical outcomes of expansive open-door laminoplasty for cervical spondylotic myelopathy. Spine (Phila PA 1976). 2003 Jun 15;28(12):1258-62. PMID:12811268 (Link to Abstract)
2. Chiba K, Ogawa Y, Ishii K, Takaishi H, Nakamura M, Maruiwa H, Matsumoto M, Toyama Y. Long-term results of expansive open-door laminoplasty for cervical myelopathy--average 14-year follow-up study. Spine (Phila PA 1976). 2006 Dec 15;31(26):2998-3005. PMID:17172996 (Link to Abstract)
(OBQ10.163) Which of the following variables has the strongest association with poor clinical outcomes in patients who undergo expansive laminoplasty for cervical spondylotic myelopathy? Review Topic
Fixed cervical kyphosis is associated with poor functional outcomes when performing an expansive laminoplasty for cervical spondylotic myelopathy.
Suda et al performed a retrospective study of 111 patient who underwent canal expanding laminoplasty for cervical myelopathy. The found a local kyphosis of > 13 degrees and signal intensity change on MRI were the most crucial risk factors for poor surgical outcomes. In patients with local kyphosis exceeding 13°, they recommend anterior decompression with correction of kyphosis in addition to posterior decompression.
Chiba et al reviewed the long-term results of open-door laminoplasty for cervical myelopathy. They found satisfactory results of open-door laminoplasty at an average follow up of 14 years. They found patients with preoperative kyphosis in the OPLL group had much lower recovery rates than those with lordotic and straight alignments, although statistical significance was not detected due to the small sample size.
Incorrect Answers: Answer 1: Laminoplasty is effective at decompressing multiple stenotic levels, and therefore multi-level stenosis is not associated with poor outcomes. Answer 2: Although duration of symptoms and severity of symptoms have been associated with poor clinical outcomes, the Suda et al study found local kyphosis was the strongest predictor of poor clinical outcomes. Answer 4. Based on available literature osteoporosis is not a predictor of poor surgical outcomes with laminoplasty. Answer 5: While cord signal change, or myelomalacia, is associated with poor functional outcomes, CSF effacement alone is not.
1. Suda K, Abumi K, Ito M, Shono Y, Kaneda K, Fujiya M. Local kyphosis reduces surgical outcomes of expansive open-door laminoplasty for cervical spondylotic myelopathy. Spine (Phila Pa 1976). 2003 Jun 15;28(12):1258-62. PMID:12811268 (Link to Abstract)
2. Chiba K, Ogawa Y, Ishii K, Takaishi H, Nakamura M, Maruiwa H, Matsumoto M, Toyama Y. Long-term results of expansive open-door laminoplasty for cervical myelopathy--average 14-year follow-up study. Spine (Phila Pa 1976). 2006 Dec 15;31(26):2998-3005. PMID:17172996 (Link to Abstract)
Fasciculations are a clinical sign of a lower motor neuron disorders. The lower motor neuron is defined as the nerve fibers traveling from the anterior horn of the spinal cord to the peripheral muscle. Lesions to the lower motor neuron are characterized by fasciculations and flaccid paralysis. The upper motor neuron is defined as the nerve fibers traveling from the motor cortex of the brain to the anterior horn of the spinal cord. Upper motor neuron disorders are characterized by spastic paralysis, exaggerated deep tendon reflexes, sustained clonus, and an up-going Babinski sign. Muscle weakness is a clinical sign of both upper and lower motor neuron disorders.
REFERENCES:
1. Einhorn TA, O’Keefe RJ, Buckwalter JA (eds): Orthopaedic Basic Science: Foundations of Clinical Practice, ed 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2007, pp 427-443
2. Renshaw TS, Deluca PA: Cerebral palsy, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics. Philadelphia, PA, Lippincott Williams & Wilkins, 2006, pp 551-603
(OBQ08.106) Following a C3-C7 laminoplasty in a myelopathic patient with cervical stenosis, the most common neurologic complication would manifest with which of the following new postoperative exam findings Review Topic
A C5 palsy (deltoid and biceps weakness) is the most likely neurologic complication following cervical laminoplasty, with an incidence of ~5%. Its pathogenesis and the options for prevention and treatment remain unidentified and many controversies exist. Two theories to account for the pathogenesis of C5 palsy exist: 1) nerve root injury 2) segmental spinal cord disorder. Neither of these hypotheses has been consistently supported and evidence to refute each hypothesis can be found in the literature. Although patients with C5 palsy generally have a good prognosis for neurologic and functional recovery, those with severe paralysis require significantly longer recovery times when compared to more mild cases.
Sakaura et report a 4.6% incidence of postoperative C5 palsy. They found no significant difference between patients undergoing anterior decompression and fusion and posterior laminoplasty. There was also no difference between cervical spondylotic myelopathy and ossification of the posterior longitudinal ligament.
Chiba et al found the pattern of delayed onset of paralysis, dysesthesia in the upper extremities, and the presence of T2 high-signal intensity zones suggest that a certain impairment in the gray matter of the spinal cord may play an important role in the development of postoperative segmental motor paralysis.
Kaneko et al attempted to investigate the possible mechanism for postoperative motor dominant C5 paralysis from intraoperative electrophysiological studies. They found a 7.6% incidence of postoperative motor dominant C5 paralysis. C5 paralysis occurred from 1 to 3 days after surgery and compromised unilaterally in all 5 patients. They were unable to draw significant conclusions regarding the etiology.
Incorrect Answers: Answer 1: Change in voice and difficulty swallowing is associated with a recurrent laryngeal nerve injury, which is associated with anterior procedures and not a posterior laminoplasty. Answer 2: Although a C7 palsy (triceps weakness) is a possible complication of a laminoplasty, a C5 palsy is more common. Answer 3: A hypoglossal nerve injury is a rare complication of anterior cervical surgery and results in deviation of the tongue Answer 4: Horner's syndrome is a rare complication of anterior cervical surgery, and presents with ptosis, miosis, and anhidrosis.
REFERENCES:
1. Kaneko K, Hashiguchi A, Kato Y, et al: Investigation of motor dominant C5 paralysis after laminoplasty from the results of evoked spinal cord lesions. J Spinal Disord Tech 2006; 19:358-361 PMID:16826009 (Link to Abstract)
2. Sakaura H, Hosono N, Mukai Y, et al: C5 palsy after decompression surgery for cervical myelopathy: Review of the literature. Spine 2003; 28:2447-2451 PMID:14595162 (Link to Abstract)
3. Chiba K, Toyama Y, Matsumoto M, et al: Segmental motor paralysis after expansive open-door laminoplasty. Spine 2002; 27:2108-2115 PMID:12394922 (Link to Abstract)
(OBQ08.131) A 56-year-old male presents with gait imbalance and decreased manual dexterity. Sagittal T2 MRI images are shown in Figures A and B. What is the most appropriate surgical management? Review Topic
The patient in this scenario is suffering from cervical spondylotic myelopathy, as they are experiencing decreased manual dexterity and likely an ataxic shuffling gait. MRI shows a narrowed canal with significant spinal cord compression and myelomalacia (spinal cord signal on T2 images). In addition, as seen in the second image, the patient has greater than 10 degrees of kyphosis.
Geck et al review the surgical treatment options for myelopathy. Myelopathy with motor/gait impairment is a surgical indication. The question they are testing is whether to do an anterior or posterior decompression. Kyphosis of > 10 degrees is a contraindication to posterior decompression, making the correct choice to be answer 2, anterior decompression and fusion. Per the cited article, the indications for an ACDF include cervical myelopathy from soft disc herniation or from spondylitic degeneration that is limited to the disc level (for one to two level spondylosis without retrovertebral disease). If there is compression behind the body from migrated disc fragments or from ossification of the PLL (retrovertebral disease), then another operation should be performed; usually an anterior corpectomy and strut grafting will enable better decompression and is ideal for patients with kyphosis or neck pain. Laminectomy historically has poor results from late deformity and late neurologic deterioration. Laminoplasty was developed to address cervical stenosis of THREE or more segments, and compares favorably with anterior corpectomy and fusion for neurologic recovery. Laminoplasty does have a lower complication rate than corpectomy and strut grafting, but has a higher incidence of postop axial symptoms.
REFERENCES:
1. Geck MJ, Eismont FJ: Surgical options for the treatment of cervical spondylotic myelopathy. Orthop Clin Northo Am 2002;33:329-348 PMID:12389279 (Link to Abstract)
(OBQ07.45) A 67-year-old woman presents with low back pain and bilateral buttock and leg pain. She prefers to stoop over the shopping cart whenever shopping. She recently noticed difficulty picking up small objects and buttoning her shirt. Physical exam shows normal strength in her lower extremities, and 3+ bilateral patellar reflexes. Gait examination shows a broad, unsteady gait. Flexion and extension radiographs of the lumbar spine are shown in Figure A and B. A lumbar MRI is shown in Figure C. What is the most appropriate next step in management? Review Topic
The patient is exhibiting signs and symptoms of lumbar spinal stenosis, which is confirmed by lumbar stenosis seen on her lumbar MRI. However, she also has clincial symptoms of cervical myelopathy. Therefore the next step in management is to obtain an MRI of the cervical spine.
Epstein et al discussed how to approach patients that are symptomatic from both cervical and lumbar spinal stenosis. They found cervical cord decompression often resulted in improvement in lumbar symptoms with resolution of pain, spasticity, and sensory deficits of myelopathic origin. They also found after cervical laminectomy, myelopathy improved or stabilized, and the subsequent lumbar decompression could be completed with less risk.
Laroche et al looked at the frequency of association between lumbar and cervical stenosis. They found 10 out of the 17 patients having cervical myelopathy had lumbar spinal stenosis as evidenced by sagittal tomography and/or computerized tomography. 9 out of the 30 patients admitted for symptomatic lumbar spinal stenosis had coexisting cervical canal stenosis as evidenced by sagittal tomography.
Incorrect Answers: Answer 1: The symptoms of cervical myelopathy take precedence, and therefore an MRI of the cervical spine should be performed prior to proceeding with lumbar surgery. Answer 2: (same as answer 1) Answer 3: A discogram is not indicated for the management of spinal stenosis or cervical myelopathy. Answer 5: While a lumbar epidural injection is a viable treatment option for spinal stenosis, the patient has symptoms of cervical myelopathy that must be investigated.
REFERENCES:
1. Epstein NE, Epstein JA, Carras R, Murthy VS, Hyman RA. Coexisting cervical and lumbar spinal stenosis: diagnosis and management. Neurosurgery. 1984 Oct;15(4):489-96. PMID:6493458 (Link to Abstract)
2. Laroche M, Moulinier L, Arlet J, Arrue P, Rousseau H, Cantagrel A, Mazieres B. Lumbar and cervical stenosis. Frequency of the association, role of the ankylosing hyperostosis. Clin Rheumatol. 1992 Dec;11(4):533-5. PMID:1486746 (Link to Abstract)
(OBQ07.180) A 63-year-old female presents with a broad-based shuffling gait, loss of manual dexterity, and exaggerated deep tendon reflexes in the lower extremities. A T2-weighted MRI scan is shown in Figure A. What is the most appropriate treatment? Review Topic
The patient has spondylotic cervical myelopathy with progressive neurologic symptoms, so surgical decompression is indicated. Imaging shows kyphotic alignment, so the most appropriate treatment is with an anterior procedure to restore alignment to neutral or lordosis. This could be done either be a C6 corpectomy or multi-level ACDF.
In patients with cervical spondylotic myelopathy the choice between an anterior, posterior, or combined approach is based primarily on: (1) the sagittal alignment of the spinal column, (2) levels involved (3) location of compression, (4) preoperative neck pain, and (5) previous operations, and (6) status of RLN. In patients with cervical kyphosis the spinal cord is pulled anteriorly against the anterior degenerative structures. Therefore, in patients with rigid kyphosis of > 10 degrees an anterior procedure is required to address the anterior compressive structures.
Kawakami et al is a retrospective cohort study (LOE-3) that compared surgical outcomes for 136 patients who underwent anterior or poster multi-level fusions for cervical myelopathy. They found that those patients with kyphotic cervical spines had inferior results to those who had lordotic or straight alignment and suggested maintaining or improving lordosis during surgery to improve outcome
Rao et al is a review article examining multiple treatment modalities for cervical spondylotic myelopathy. They state that anterior approaches can be performed for single or multi-level procedures and that anterior approaches are preferred for those patients who have loss of cervical lordosis.
Figure A shows A T2-weighted MRI with multi-level compression, worse at C5/6 and C6/7, in a patient with cervical kyphosis. Illustration A shows how to measure the C2-C7 sagittal alignment and focal sagittal alignment in this patient. Illustration B shows how in a kyphotic spine, why a laminectomy fails to address the anterior compression on the spinal cord.
Incorrect Answers: Answer 1-3: In this case posterior decompression alone is contraindicated because the patient is kyphotic. Posterior decompression alone will not allow posterior translation of the spinal cord away from the anterior compressive pathology, which can only be done by correcting the kyphotic deformity. Answer 5: Immobilization in halo will not decompress the spine nor correct the kyphotic deformity. In the setting of myelopathy and progressive neurological deterioration, spinal decompression should be considered.
1. Kawakami M, Tamaki T, Iwasaki H, Yoshida M, Ando M, Yamada H. A comparative study of surgical approaches for cervical compressive myelopathy. Clin OrthopRelat Res. 2000 Dec;(381):129-36. PMID:11127649 (Link to Abstract)
2. Rao RD, Gourab K, David KS. Operative treatment of cervical spondylotic myelopathy. J Bone Joint Surg Am. 2006 Jul;88(7):1619-40. PMID:16818991 (Link to Abstract)
(OBQ07.189) In patients with symptoms of cervical myelopathy, what variable is associated with improved outcomes with nonoperative management? Review Topic
1. Increased Central Motor Conduction Time (CMCT)
3% (23/677)
2. Transverse area of the spinal cord >70mm2
61% (411/677)
3. Isolated low intramedullary signal on T1WI
5% (32/677)
4. A midsagittal diameter of the spinal canal of <13mm
In patients with cervical myelopathy, nonoperative management is most likely to be successful when there is a larger transverse area of the spinal cord.
In patients with physical exam findings and symptoms of cervical myelopathy, surgical treatment is usually indicated. There may be a subset of patients with mild symptoms that do better with nonoperative treatment, although the specific indications for nonoperative treatment remains controversial. The Japanese Orthopaedic Association (JOA) classification system is frequently used to measure the severity of symptoms. It is a 17 point scoring system based on: 1) upper extremity function, 2) lower extremity function 3) sensory function 4) bladder function. A score of 17 is normal.
Kadanka et al. compared conservative and surgical treatment of spondylotic cervical myelopathy. They found patients who had good outcomes with conservative treatment were older in age, had normal central motor conduction time (CMCT), and had a larger transverse area of the spinal cord (>70mm2).
Rao et al. report surgical treatment is indicated for most patients with clinically evident cervical spondylotic myelopathy. They state patients with very early or mild clinical findings should be clinically and radiographically assessed with regard to their level of disability, the duration of symptoms, the degree of stenosis, and evidence of progression. A decision regarding treatment is made by weighing these factors against the risks of operative treatment.
Wada et al. looked at the long term outcomes of surgical treatment and the association with the JOA score. They recommend operative treatment when there is a JOA score of <13 points and spinal cord compression on imaging studies.
Illustration A is a table showing the JOA classification and scoring system. Illustration B shows the different radiographic measurements Rao et al. recommend to evaluate cervical myelopathy.
Incorrect Answer: Answer 1: Increased central motor conduction time (CMCT) would be a poor prognostic indicator for nonoperative treatment. Answer 3: Isolated low intramedullary signal on T1WI are thought to represent cord edema or irreversible changes such as gliosis or microcavitation and are likely to show little improvement with conservative OR surgical interventions. Answer 4: Per the discussion above, a midsagittal diameter of the spinal canal of <13mm would be a poor prognostic indicator for nonoperative treatment. Answer 5: According to Kadanka et al, older patients do better with nonoperative management.
1. Kadanka Z, Mares M, Bednarík J, Smrcka V, Krbec M, Chaloupka R, Dusek L. Predictive factors for spondylotic cervical myelopathy treated conservatively or surgically. Eur J Neurol. 2005 Jan;12(1):55-63. PMID:15613148 (Link to Abstract)
2. Rao RD, Gourab K, David KS. Operative treatment of cervical spondylotic myelopathy. J Bone Joint Surg Am. 2006 Jul;88(7):1619-40. PMID:16818991 (Link to Abstract)
3. Wada E, Suzuki S, Kanazawa A, Matsuoka T, Miyamoto S, Yonenobu K. Subtotal corpectomy versus laminoplasty for multilevel cervical spondylotic myelopathy: a long-term follow-up study over 10 years. Spine (Phila Pa 1976). 2001 Jul 1;26(13):1443-7; discussion 1448. PubMed PMID: 11458148. PMID:11458148 (Link to Abstract)
(OBQ05.92) Postoperative radiculopathy is a known complication of posterior cervical decompression for myelopathy. One potential mechanism of nerve root injury is thought to be tethering of the nerve root with dorsal migration of the spinal cord. What is the most common radicular pattern seen with this condition? Review Topic
1. Motor-dominant radiculopathy with weakness of the deltoid
59% (734/1239)
2. Sensory-dominant radiculopathy with pain in the lateral shoulder
22% (274/1239)
3. Motor-dominant radiculopathy with weakness of the wrist extensors
6% (79/1239)
4. Sensory-dominant radiculopathy with pain in the lateral forearm
9% (115/1239)
5. Motor-dominant radiculopathy with weakness of the triceps
The study by Dai et al retrospectively reviewed 287 consecutive patients with cervical compression myelopathy who had been treated by multilevel cervical laminectomy and identified 37 (12.9%) with postoperative radiculopathy. The diagnosis was either cervical spondylosis (25 patients) or ossification of the posterior longitudinal ligament (12 patients). Radiculopathy was observed from four hours to six days after surgery. The most frequent pattern of paralysis was involvement of the C5 roots of the motor-dominant type. They argue, in support of prior studies by Tsuzuki et al, that postoperative radiculopathy is caused by a tethering injury to the root caused by of expansion and dorsal migration of the spinal cord rather than a technical problem.
REFERENCES:
1. Dai L, Ni B, Yuan W, Jia L. Radiculopathy after laminectomy for cervical compression myelopathy. J Bone Joint Surg Br. 1998 Sep;80(5):846-9. PMID:9768896 (Link to Abstract)
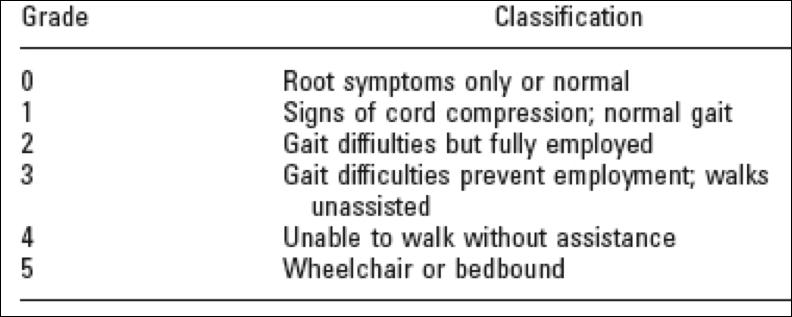
The Nurick Classification system is a classification system for cervical myelopathy that focuses on the ambulatory status of the patient.
The different Grades of the Nurick classification system include: (GRADE 0) Signs or symptoms of root involvement but without evidence of spinal cord disease. (GRADE 1) Signs of spinal cord disease but no difficulty in walking. (GRADE 2) Slight difficulty in walking that did not prevent full-time employment. (GRADE 3) Difficulty in walking that prevented full-time employment or the ability to perform all housework but that was not severe enough to require someone else’s help to walk. (GRADE 4) Able to walk with someone else’s help or the aid of a frame. (GRADE 5) Chair bound or bedridden.
Hirabayashi et al present a Level 4 study of 53 cases who underwent surgical decompression for patients with OPLL and concomitant myelopathy or radiculopathy. They reported a recovery rate of approximately 70%.
Edwards et al present a Level 5 review of cervical myelopathy. They report that anterior decompression and fusion procedures including 1 or 2 levels have predictable results, but ACDFs involving 3 or more levels are associated with increased morbidity.
Illustration A describes the Nurick Classification system in chart format.
Incorrect Answers: Answer 2: The Japanese Orthopaedic Association Classification system includes chopstick function. Answer 3: The Modified Japanese Orthopaedic Association Classification system includes upper extremity dexterity tasks such as buttoning of a shirt. Answer 4: The Ranawat Classiciation takes into account upper extremity, and well as lower extremity, symptoms. Answer 5: The Oswestry Disability Index is a classification for back pain, not cervical myelopathy.
1. Nurick S: The natural history and the results of surgical treatment of the spinal cord disorder associated with cervical spondylosis. Brain 1972:95:101-108 PMID:5023079 (Link to Abstract)
2. Hirabayashi K. Miyakawa J, Satomi K, et al: Operative results and postoperative progression of ossification among patients with ossification of cervical posterior longitudinal ligament. Spine 1981:6:354-364 PMID:6792717 (Link to Abstract)
3. Edwards CC IL, Riew KD, Anderson PA, et al: Cervical myelopathy: Current diagnostic and treatment strategies. Spine J 2003:3:68-81 PMID:14589250 (Link to Abstract)
(OBQ04.61) A 66-year-old male presents with neck pain, difficulty with fine motor activities like buttoning shirts, and mild gait instability. On physical examination he has 5 of 5 motor strength in all muscles groups in his upper and lower extremities, a bilateral Hoffman sign, bilateral 3+ patellar reflexes, 3 beats of clonus on the right, and no clonus on the left. Radiographs show segmental kyphosis of 12 degrees from C4 to C7. MRI shows circumferential compression at C5/6 with complete effacement of CSF and T2 intramedullary signal. What is the most accurate description of how his symptoms will progress over time? Review Topic
1. Stable over time.
4% (38/845)
2. Improvement following a course of high-dose IV spinal steroids.
3% (28/845)
3. Improvement following a period of rest, physical therapy, and oral medication.
2% (18/845)
4. Slow progression in a pattern of stepwise deterioration following periods of stable symptoms.
81% (681/845)
5. Rapid and serious deterioration requiring urgent surgical treatment.
The natural history of spondylotic cervical myelopathy is characterized by slow progression in a pattern of stepwise deterioration following periods of stable symptoms. Factors that are associated with worse outcomes with nonoperative treatment include segmental kyphosis and circumferential compression spinal cord compression. Whether T2 signal intensity predicts progression is controversial.
Clarke et al, in a historic article from 1974, found "where subsequent extension of the disease occurred, it was often very slow."
Lees et al in another historic article report that in patients with CSM the natural history is characterized by "periods of long non-progressive disability."
Shimomura et al looked at factors that could predict progression in patients with CSM. They found patients with circumferential spinal cord compression in the maximum compression segment on axial MRI tended to do worse with nonoperative treatment.
Oshima et al also looked at factors that could predict progression in patients with CSM. They found segmental kyphosis and instability at the narrowest canal were considered to be adverse prognostic factors with nonoperative treatment.
Emery in a review article reports "the natural history of this disorder is usually slow deterioration in a stepwise fashion, with worsening symptoms of gait abnormalities, weakness, sensory changes, and often pain. Minimal symptoms without hard evidence of gait disturbance or pathologic reflexes warrant nonoperative treatment, but patients with demonstrable myelopathy and spinal cord compression are candidates for operative intervention."
REFERENCES:
1. Clarke E, Robinson PK. Cervical myelopathy: a complication of cervical spondylosis. Brain. 1956 Sep;79(3):483-510. PMID:13364095 (Link to Abstract)
2. Emery SE. Cervical spondylotic myelopathy: diagnosis and treatment. J Am Acad Orthop Surg. 2001 Nov-Dec;9(6):376-88. Review. PMID:11767723 (Link to Abstract)
3. Lees F, Turner JW. Natural history and prognosis of cervical spondylosis. Br. Med J. 1963 Dec 28;2(5373):1607-10. PMID:14066179 (Link to Abstract)
4. Shimomura T, Sumi M, Nishida K, Maeno K, Tadokoro K, Miyamoto H, Kurosaka M, Doita M. Prognostic factors for deterioration of patients with cervical spondylotic myelopathy after nonsurgical treatment. Spine (Phila Pa 1976). 2007 Oct 15;32(22):2474-9. PubMed PMID: 18090088. PMID:18090088 (Link to Abstract)
5. Oshima Y, Seichi A, Takeshita K, Chikuda H, Ono T, Baba S, Morii J, Oka H, Kawaguchi H, Nakamura K, Tanaka S. Natural Course and Prognostic Factors in Patients with Mild Cervical Spondylotic Myelopathy with Increased Signal Intensity on T2-weighted Magnetic Resonance Imaging. Spine (Phila Pa 1976). 2012 Apr 14. [Epub ahead of print] PubMed PMID: 22511231. PMID:22511231 (Link to Abstract)
(OBQ04.205) A 35-year-old man complains of clumsiness when buttoning his shirt and frequent episodes of falling when ambulating. Further work-up reveals congenital cervical spinal stenosis with spinal cord compression. Because of his young age, posterior laminoplasty is performed. Which nerve root is most likely to be adversely affected following surgery? Review Topic
Neurologic deterioration during and after surgery is one of the most serious complications of surgery for cervical compression myelopathy. The earliest article (Yonenobu Spine 1991) looked at 384 patients over 18 years who underwent surgery for cervical myelopathy. Neurologic deterioration was found in 21 patients (5.5%). 13 of these showed signs of C5 root paresis while 8 showed signs of spinal cord dysfunction. While an etiology could be described for 4 of the patients with C5 root paresis (3 graft displacement, 1 hyperextension), the etiology of the remaining 9 was unknown. Even CT myelography could only offer the possible explanation of acute large shift of the spinal cord as being responsible for these defects. Myelograms of 25 patients without neurologic complications showed the maximum cord shift was at C5, but the average shift was not any different from patients with complications. Further studies have corroborated the observances of the 1991 study showing that the C5 root is most affected by postoperative paralysis following posterior cervical decompression. The 2002 paper suggested that in an effort to reduce postoperative C5 nerve root palsy, the clinician should consider intraoperative deltoid and biceps transcranial electrical motor-evoked potential and spontaneous electromyography monitoring whenever there is potential for iatrogenic C5 nerve root injury. They were able to detect injury prospectively and avert more serious consequences with intraoperative monitoring.
REFERENCES:
1. Fan D, Schwartz DM, Vaccaro AR, Hilibrand AS, Albert TJ. Intraoperative neurophysiologic detection of iatrogenic C5 nerve root injury during laminectomy for cervical compression myelopathy. Spine (Phila Pa 1976). 2002 Nov 15;27(22):2499-502. PMID:12435981 (Link to Abstract)
2. Dai L et al. Radiculopathy after laminectomy for cervical compression myelopathy. JBJS-B 1998;80:846-849 PMID:9768896 (Link to Abstract)
3. Yonenobu K et al. Neurologic complications of surgery for cervical compression myelopathy. Spine 1991;16:1277-1282 PMID:1750000 (Link to Abstract)
(OBQ04.207) A 45-year-old man presents to your office with difficulty ambulating and buttoning his shirt. It started two years ago but has worsened significantly over the last year. On physical exam he is unable to perform a tandem gait and has a positive Hoffman's sign bilaterally, however he has no clonus and a down-going babinski bilaterally. He has 4/5 strength in his hands, but 5/5 strength in all other muscle groups. Figure A is a sagittal MRI. Figures B and C are an axial MRI cuts through C4/5 and C5/6, respectively. What is the appropriate next step? Review Topic
The clinical picture is consistent with progressive cervical myelopathy, and the best treatment option is an anterior cervical discectomy and fusion. Because there is compression at C4/5 and C5/6, an ACDF would need to be done at both levels.
The patient has signs and symptoms of progressive myelopathy, such as difficulty with tandem gait, buttoning his shirt, and positive Hoffman's reflexes. While the patient does not have all the classic positive signs (i.e. the patient has no clonus and down-going Babinski signs), a diagnosis of myelopathy does not require all signs be present. Furthermore, the imaging studies demonstrate significant cord compression behind the C4/5 and C5/6 intervertebral disc. The best treatment is an ACDF.
Rhee et al. reported on the prevalence of myelopathic signs in patients with known myelopathy. They reported that 79% of patients demonstrated at least one myelopathic sign, with a Hoffman's sign being the most common (59%). Comparatively, an up-going Babinski sign and clonus were each only present in 13% of patients with myelopathy.
Herkowitz et al. reported similar efficacy when treating patients with a cervical disc herniations either from the front with an anterior cervical discectomy and fusion, or from the back with a posterior cervical laminotomy-foraminotomy. However, all patients with myelopathy and midline compression (like the patient in the current question) underwent an ACDF.
Figure A is a sagittal T2 MRI demonstrating cord compression at the C4/5 and C5/6 level, and Figures B and C demonstrates cord compression on the axial series.
Incorrect Answers Answers 1-3: These are all non-operative treatments. Given that the patient is having progressive cervical myelopathy, there is no further indication for non-operative care. Answer 5: Posterior cervical laminotomy-foraminotomy would not adequately decompress the spinal cord.
REFERENCES:
1. Rhee JM, Heflin JA, Hamasaki T, Freedman B. Prevalence of physical signs in cervical myelopathy: a prospective, controlled study. Spine (Phila Pa 1976). Apr 20 2009;34(9):890-895 PMID:19352222 (Link to Abstract)
2. Herkowitz HN, Kurz LT, Overholt DP. Surgical management of cervical soft disc herniation. A comparison between the anterior and posterior approach. Spine(Phila Pa 1976). 1990 Oct;15(10):1026-30. PMID:2263967 (Link to Abstract)
Harrop JS, Naroji S, Maltenfort M, Anderson DG, Albert T, Ratliff JK, Ponnappan RK, Rihn JA, Smith HE, Hilibrand A, Sharan AD, Vaccaro A Spine. 2010 Mar;35(6):620-4. PMID: 20150835 (Link to Pubmed)
Oshima Y, Seichi A, Takeshita K, Chikuda H, Ono T, Baba S, Morii J, Oka H, Kawaguchi H, Nakamura K, Tanaka S Spine. 2012 Oct;37(22):1909-13. PMID: 22511231 (Link to Pubmed)














 Review Topic
Review Topic 











 The patient is a 51 year old female with a significant psych history who I...
The patient is a 51 year old female with a significant psych history who I... 









Question Comments