Pediatric Mononucleosis and Epstein-Barr Virus Infection
- Author: Nicholas John Bennett, MBBCh, PhD, MA(Cantab), FAAP; Chief Editor: Russell W Steele, MD more...
Updated: May 12, 2015
Background
Epstein-Barr virus (EBV), or human herpesvirus 4, is a gammaherpesvirus that infects more than 95% of the world's population. The most common manifestation of primary infection with this organism is acute infectious mononucleosis, a self-limited clinical syndrome that most frequently affects adolescents and young adults. Classic symptoms include sore throat, fever, and lymphadenopathy. Infection with Epstein-Barr virus in younger children is usually asymptomatic or mild. However, Epstein-Barr virus is also a human tumor virus, the first virus associated with human malignancy. Infection with Epstein-Barr virus is associated with lymphoproliferative disorders, especially in immunocompromised hosts, and is associated with various tumors, including nasopharyngeal carcinoma and Burkitt lymphoma.
See Clues in the Oral Cavity: Are You Missing the Diagnosis?, a Critical Images slideshow, to help identify the causes of abnormalities of the oral cavity.
Acute infectious mononucleosis was first described in the late 19th century as acute glandular fever, an illness consisting of lymphadenopathy, fever, hepatosplenomegaly, malaise, and abdominal discomfort in adolescents and young adults. In 1920, Sprunt and associates applied the name infectious mononucleosis to cases of spontaneously resolving acute leukemia associated with blastlike cells in the blood. Downey described the lymphocyte morphology in 1923. In 1932, Paul and Bunnell discovered that serum from symptomatic patients had antibodies that agglutinate the RBCs of unrelated species, the heterophile antibodies. This allowed enhanced diagnostic accuracy of infectious mononucleosis. The graph below demonstrates the antibody response to Epstein-Barr virus.
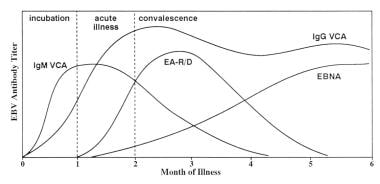 Infectious mononucleosis. Antibody response to Epstein-Barr virus. Adapted with permission from Johnson DH, Cunha BA. Epstein-Barr virus serology. Infect Dis Pract. 1995;19:26-27.
The search for the etiologic agent of infectious mononucleosis was unsuccessful for many years, partly because researchers did not appreciate that most primary infections are asymptomatic and that most adults are seropositive. In 1964, Epstein described the first human tumor virus when he found virus particles in a Burkitt lymphoma cell line.[1] Henle reported the relationship between acute infectious mononucleosis and Epstein-Barr virus in 1968.[2] Subsequently, a large prospective study of students at Yale University firmly established Epstein-Barr virus as the etiologic agent of infectious mononucleosis.[3]
Infectious mononucleosis. Antibody response to Epstein-Barr virus. Adapted with permission from Johnson DH, Cunha BA. Epstein-Barr virus serology. Infect Dis Pract. 1995;19:26-27.
The search for the etiologic agent of infectious mononucleosis was unsuccessful for many years, partly because researchers did not appreciate that most primary infections are asymptomatic and that most adults are seropositive. In 1964, Epstein described the first human tumor virus when he found virus particles in a Burkitt lymphoma cell line.[1] Henle reported the relationship between acute infectious mononucleosis and Epstein-Barr virus in 1968.[2] Subsequently, a large prospective study of students at Yale University firmly established Epstein-Barr virus as the etiologic agent of infectious mononucleosis.[3]
See Clues in the Oral Cavity: Are You Missing the Diagnosis?, a Critical Images slideshow, to help identify the causes of abnormalities of the oral cavity.
Acute infectious mononucleosis was first described in the late 19th century as acute glandular fever, an illness consisting of lymphadenopathy, fever, hepatosplenomegaly, malaise, and abdominal discomfort in adolescents and young adults. In 1920, Sprunt and associates applied the name infectious mononucleosis to cases of spontaneously resolving acute leukemia associated with blastlike cells in the blood. Downey described the lymphocyte morphology in 1923. In 1932, Paul and Bunnell discovered that serum from symptomatic patients had antibodies that agglutinate the RBCs of unrelated species, the heterophile antibodies. This allowed enhanced diagnostic accuracy of infectious mononucleosis. The graph below demonstrates the antibody response to Epstein-Barr virus.
Infectious mononucleosis. Antibody response to Epstein-Barr virus. Adapted with permission from Johnson DH, Cunha BA. Epstein-Barr virus serology. Infect Dis Pract. 1995;19:26-27.
No comments:
Post a Comment