Trouble With The Curve – Solved
- October 8, 2012 – 12:00 am
- Posted in Atlas Subluxation, Chiari Malformation, Quality of Life, spinal epigenetics, Stability and Structure, TMJ Dysfunction, Uncategorized, X-ray Quality
- Comments (10)
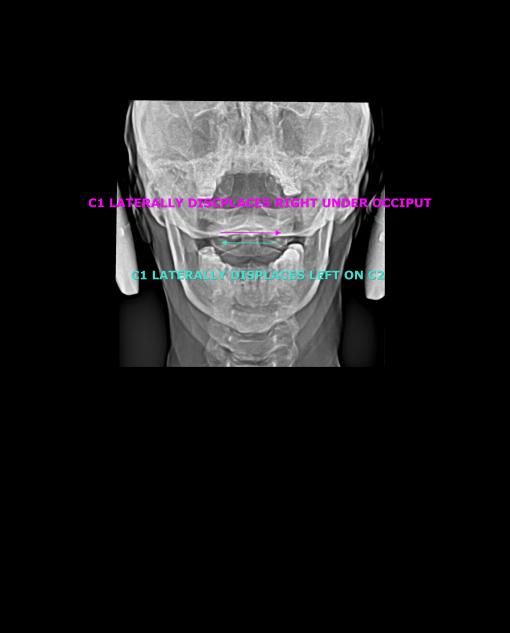
A young woman presented last week, having been told by her primary care physician that a reverse curve really wouldn’t cause her milieu of problems. (Neck pain, neck stiffness, decreased range of motion, dizziness, “foggy-thinking”, jaw pain, poor sleep, headaches, etc.) She then sought out the care of a chiropractor, who proceeded to assure her that her reversed curve was so bad that she would just have to live with it–and, see him once a week for the rest of her life just to make it bearable. (get used to it, and pay…) Desperate, worried and in tears we spoke on her first visit. I looked at her x-rays, and thought… “I think I can help this woman” (….but then again, I have thoughts like this all the time….)
After examination, I told her that it was quite likely that she had an atlas subluxation–and I thought she was a candidate for the atlas positioning procedure. We obtained useful images which confirmed the diagnosis of Atlas Subluxation, and we scheduled the procedure. She returned several days later. Immediately following the procedure, I could see the life return to her face, she took a deep breath, and smiled at me.. and I thought, “oh… so this is what you look like” She spent her next 30 minutes recovering and stabilizing in my recovery area. When she arose, I post checked her and re-imaged her. The post x-rays told the story: she had embarked upon the healing path. She knew it. I knew it. I love my work.
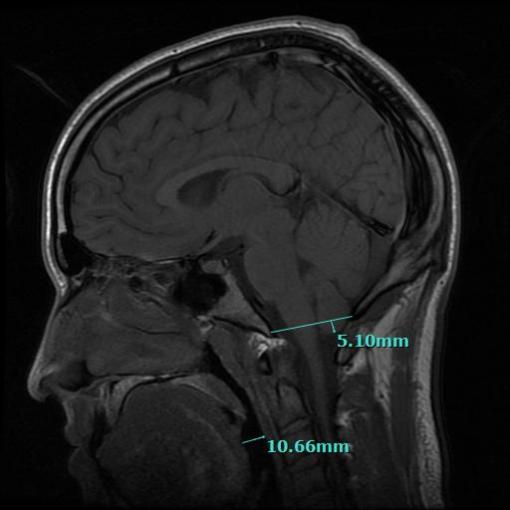
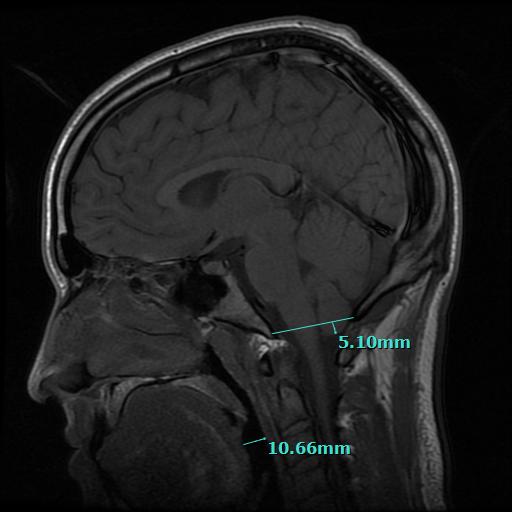
Curious about her immediate relief, I asked to see an MRI of her head and neck which was taken prior to her initial visit in my office. I suspected that the cervical kyphosis was perhaps exerting a “tractioning” down force on the cerebellar tonsils, and drawing them into an aspect of the foreman magnum, thus interfering with CSF flow out of the cranial vault. Cerebellar tonsillar ectopy (CTE)is a common finding in the whiplash population according to a study done by Freeman, Rosa, et al. CTE exists when the lower part of the cerebellum abnormally extends down into the foreman magnum (the big hole at the bottom of the skull through which passes the spinal cord, the vertebral arteries and the cerebrospinal fluid.) As suspected, she did have CTE, exacerbated by the fact that her cervical spine had a reversal of the normal curvature, and a significant lateral displacement. A post MRI has not been performed yet, but in most cases wherein “pre” and “post” MRI studies have been performed following the Trans-dermal Atlas Positioning (TAP) procedure, the CTE is resolved. (See Freeman, Rosa, et al.)




After examination, I told her that it was quite likely that she had an atlas subluxation–and I thought she was a candidate for the atlas positioning procedure. We obtained useful images which confirmed the diagnosis of Atlas Subluxation, and we scheduled the procedure. She returned several days later. Immediately following the procedure, I could see the life return to her face, she took a deep breath, and smiled at me.. and I thought, “oh… so this is what you look like” She spent her next 30 minutes recovering and stabilizing in my recovery area. When she arose, I post checked her and re-imaged her. The post x-rays told the story: she had embarked upon the healing path. She knew it. I knew it. I love my work.
Curious about her immediate relief, I asked to see an MRI of her head and neck which was taken prior to her initial visit in my office. I suspected that the cervical kyphosis was perhaps exerting a “tractioning” down force on the cerebellar tonsils, and drawing them into an aspect of the foreman magnum, thus interfering with CSF flow out of the cranial vault. Cerebellar tonsillar ectopy (CTE)is a common finding in the whiplash population according to a study done by Freeman, Rosa, et al. CTE exists when the lower part of the cerebellum abnormally extends down into the foreman magnum (the big hole at the bottom of the skull through which passes the spinal cord, the vertebral arteries and the cerebrospinal fluid.) As suspected, she did have CTE, exacerbated by the fact that her cervical spine had a reversal of the normal curvature, and a significant lateral displacement. A post MRI has not been performed yet, but in most cases wherein “pre” and “post” MRI studies have been performed following the Trans-dermal Atlas Positioning (TAP) procedure, the CTE is resolved. (See Freeman, Rosa, et al.)

BEFORE

AFTER FIRST PROCEDURE


PRE
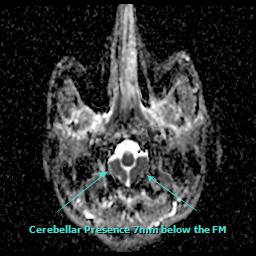
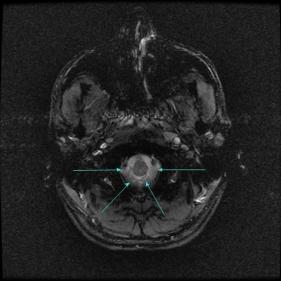
Recently, a patient flew in to see us from Germany. After a Skype interview, and my review of his MRI’s, it was determined that he was suffering symptoms from low-lying cerebellar tonsils, or, cerebellar tonsillar ectopia. This is not traditionally considered chiari malformation by many treating physicians and neuroradiologist–and not all cases are symptomatic. In this instance, the cerebellar tonsils descend seven millimeters (7mm) below the large opening at the base of the skull called the foreman magnum. The images you see below are a sagittal slice, and two horizontal slices of the patient’s brain and were taken from an MRI he received of his brain and Atlas joint in New York City at the Hospital for Special Surgery prior to coming to see us in January of 2014.
The MRI showed that the cerebellar tonsils had descended down 7mm below the opening at the base of his skull and were partially occluding the upper spinal canal.
 Chapman Clinic for Spinal and Craniofacial Epigenetics – Mild Chiari MRI of Atlas Joint
Chapman Clinic for Spinal and Craniofacial Epigenetics – Mild Chiari MRI of Atlas Joint
An excerpt from the radiology report dated February 17, 2014 after the for this patient reads:
 Symptomatic changes can occur when the head is positioned back on the top bone of the neck. Functional spaces become more capacious… Life begins to return as the body heals.
Symptomatic changes can occur when the head is positioned back on the top bone of the neck. Functional spaces become more capacious… Life begins to return as the body heals.
To schedule a consultation, call 801.655.1801
The MRI showed that the cerebellar tonsils had descended down 7mm below the opening at the base of his skull and were partially occluding the upper spinal canal.
 Chapman Clinic for Spinal and Craniofacial Epigenetics – Mild Chiari MRI of Atlas Joint
Chapman Clinic for Spinal and Craniofacial Epigenetics – Mild Chiari MRI of Atlas Joint
Chapman Clinic Mild Chiari 7mm below Foreman Magnum

Chapman Clinic Mild Chiari Presentation horizontal View
PRE-CORRECTION MRI
Views taken on January 14, 2014 in New York.
I ordered an MRI several days following the TAP AO procedure, and the cerebellar tonsils were measured at 2-3 millimeters below the skull. A remarkable 50% improvement with just one atlas correction. Following the TAP (Transdermal Atlas Positioning) procedure, the cerebellar tonsils ascended back up into the patients skull (where they below) and the symptoms immediately improved.An excerpt from the radiology report dated February 17, 2014 after the for this patient reads:
Chapman Clinic for Spinal and Craniofacial Epigenetics – Post Correction – Ordered MRI Report Excerpt
To schedule a consultation, call 801.655.1801
Hitting a Nerve – TMD (Revisited)
 We need to keep this thought in mind:
We need to keep this thought in mind:
Dental based treatment for TMJ Dysfunction and malocclusion may be enhanced by combining therapy with Atlas Aligning Chiropractic procedures known as Atlas Orthogonal. Essentially, getting one’s head on straight through specialized atlas postitioning technology can make all the difference in whether the TMJ treatment is successful or a failure.
The Atlas Orthogonal (AO) procedure can restore the essential balance and positioning of the head, neck and back–a vital part of jaw function.
Malpositions of the head and neck are often associated with a common jaw disorder called Temporomandibular Joint (TMJ) Dysfunction, or TMD. TMD is also known as TMJ Syndrome. Patients that present to a specialized dentist for TMJ treatment are often not diagnosed for craniospinal dysfunction, hence, with only half the correct diagnosis, only a partial therapeutic program is recommended.
UNDERSTANDING THE TEMPOROMANDIBULAR JOINT (TMJ):
The jaw joint is way more than a “functional hinge” joint—it is more accurately described as being suspended and “docked” in the TMJ space rather than being anchored there—much the way the boat occupies the space in a slip. In the illustration below, you can see that when the mouth is open, the head of the condyle moves down and forward. The jaw or mandible is positioned and moved by 68 pairs of muscles of the head, neck, face and shoulders, and, unlike the vast majority of other joints of the body—which remain in their location during joint range of motion—the jaw joints are compensating joints to some extent, and glide into and out of the TMJ space based on its’ natural functional movement. Therapeutically, I have found that it helps to view the tempromadibular joints as more of a biomechanical “reference point”, rather than a fixed pivot or anchor point. TMJ function, it’s neurology and ability to compensate can be a complex clinical condition.
I cannot underscore the importance of having a multidisciplinary understanding of the mandibles sophisticated behavior patterns and it’s relationships with other structures such as the atlas and the axis vertebraes (C1 and C2), as well as the 68 pairs of muscles that move and position the jaw—-this knowledge is essential when treating complex TMD.T

The good news is: Although the TMJ is very complex, it does have a simple, identifiable “axis of movement” — and that axis of motion is not in the jaw joint itself! Rather, the axis of angular rotation of the mandible is around a very important structure in cervical spine, namely, C2 vertebrae, also known as the Axis (red line). The upward jutting structure on the Axis vertebrae around which the jaw “functionally” pivots on it’s several axes is called: the “dens”. The name “dens” provides an important clue, for in Latin, dens means: “tooth”!! So, the functional axis of the jaw, and hence the dynamic pivot of occlusion, takes place around the only part of the human spine which anatomists—centuries ago I might add—dubbed the “Tooth of the Spine”… Amazing, isn’t it!?
 It has been my long experience that when the axis of something is askew, the angular movement of that part which rotates around the skewed axis also becomes irregular and skewed. Consequently, a large component of treating the irregularity of the jaw joints in their motion starts and often finishes with correctly positioning the atlas-axis joint, and specifically the dens of C2. When the motion of the jaw becomes irregular, we may experience pain and discomfort–and this is often an indication of underlying pathology such as subluxation of the atlas-axis.
It has been my long experience that when the axis of something is askew, the angular movement of that part which rotates around the skewed axis also becomes irregular and skewed. Consequently, a large component of treating the irregularity of the jaw joints in their motion starts and often finishes with correctly positioning the atlas-axis joint, and specifically the dens of C2. When the motion of the jaw becomes irregular, we may experience pain and discomfort–and this is often an indication of underlying pathology such as subluxation of the atlas-axis.
TMD Syndrome may occur when the normal functional “positions” of the jaw joints shift into irregular positions during movement and use. An uneven “grinding” or “wearing” use-pattern will likely develop, and is measurable through specialized instrumentation. This abnormal use-pattern and positioning can cause a significant amount of pain and inflammation–it can even cause tooth wear patterns, and may make chewing, sleeping, speaking and even breathing difficult.
 The pain and problems of TMD can be quite diverse. Jaw disorders can refer pain to other parts of the body–even though the jaw may not noticeably be painful itself. It can refer pain to the head, neck and upper back, the face and the teeth—–and even the entire body! This multisystem effect can cause the patient to seek out multiple practitioners for treatment for their whole body symptoms. Unfortunately, those various practitioners often find it difficult to blend their procedures with the processes and procedures of other practitioners for the good of the patient. This happens not because they are bad doctors, but because our system of healthcare does not facilitate multidisciplinary collaboration—especially between certain types of practitioners. The reasons for this sort of discord are complex in and of them selves, but I do believe—and with good reason—that this is where many TMD therapies fail.
The pain and problems of TMD can be quite diverse. Jaw disorders can refer pain to other parts of the body–even though the jaw may not noticeably be painful itself. It can refer pain to the head, neck and upper back, the face and the teeth—–and even the entire body! This multisystem effect can cause the patient to seek out multiple practitioners for treatment for their whole body symptoms. Unfortunately, those various practitioners often find it difficult to blend their procedures with the processes and procedures of other practitioners for the good of the patient. This happens not because they are bad doctors, but because our system of healthcare does not facilitate multidisciplinary collaboration—especially between certain types of practitioners. The reasons for this sort of discord are complex in and of them selves, but I do believe—and with good reason—that this is where many TMD therapies fail.
It is sort of like herding cats…
 From my clinical experience, TMD disorders, even advanced and complex cases of TMD, where vast postural compensation has occurred in the jaw muscles, occlusion, the spine and pelvis, respond well with Atlas Orthogonal treatment in conjunction with advanced dental technologies such as biomimetic occlusal therapy such as the DNA appliance. To help the reader better understand why, I have taken a few paragraphs to carefully and accurately describe the AO procedure itself.
From my clinical experience, TMD disorders, even advanced and complex cases of TMD, where vast postural compensation has occurred in the jaw muscles, occlusion, the spine and pelvis, respond well with Atlas Orthogonal treatment in conjunction with advanced dental technologies such as biomimetic occlusal therapy such as the DNA appliance. To help the reader better understand why, I have taken a few paragraphs to carefully and accurately describe the AO procedure itself.
The Atlas Orthogonal (AO) treatment is a corrective cervical spine alignment procedure performed by Board Certified Atlas Orthogonists (BCAO) chiropractic physicians.
The AO specialist utilizes 3-dimensional images (via CT or X-ray) to locate and identify abnormal malpositions of the skull, the atlas, the axis and the other 5 cervical vertebraes. Once the exact malposition has been mapped out in 3-D space, a biomechanical analysis protocol is used to derive a mathematically formulated vector.
 This vector is programmed into an corrective instrument which is designed to transfer a mechanical wave into the atlas vertebrae. The procedure is performed when the doctor precisely places the instrument against the skin over the atlas, scarcely dimpling the contact point. The doctor activates the electromagnetic magnetic driver, which produces 1.6 pounds of force. The mechanical wave is transferred through the stylus into the atlas vertebra. (I have named this the T.A.P procedure–Transdermal Atlas Positioning)
This vector is programmed into an corrective instrument which is designed to transfer a mechanical wave into the atlas vertebrae. The procedure is performed when the doctor precisely places the instrument against the skin over the atlas, scarcely dimpling the contact point. The doctor activates the electromagnetic magnetic driver, which produces 1.6 pounds of force. The mechanical wave is transferred through the stylus into the atlas vertebra. (I have named this the T.A.P procedure–Transdermal Atlas Positioning)
 The directional wave interacts with the atlas causing this structure to transfer the energy to the adjacent vertebrae to some extent which causes them to shift their position. The primary objective of the mechanical wave is to reposition the atlas vertebrae and restore it’s alignment with cervical spine and the skull. The force is gentle, and very specific as to amplitude, duration and direction. Following the procedure, the patient is physically re-examined, and, if found improved, post-imaging is performed to map out and quantify changes in the position of the atlas, occiput, axis and the cervical spine. If alignment (orthogonality) has been achieved, then the procedure is complete.
The directional wave interacts with the atlas causing this structure to transfer the energy to the adjacent vertebrae to some extent which causes them to shift their position. The primary objective of the mechanical wave is to reposition the atlas vertebrae and restore it’s alignment with cervical spine and the skull. The force is gentle, and very specific as to amplitude, duration and direction. Following the procedure, the patient is physically re-examined, and, if found improved, post-imaging is performed to map out and quantify changes in the position of the atlas, occiput, axis and the cervical spine. If alignment (orthogonality) has been achieved, then the procedure is complete.
A Sample of our Multidisciplinary Schedule on Week One
Day One:
1. Paperwork:
a. General Medical
b. Dental
2. Dr. Chapman –
a. History
b. Examination; CROM; vitals
c. Evaluation
d. Tekscan –Matscan
e. Radiographs/Cone Beam CT
f. Differential Diagnosis
3. Dr. Preble –
a. History
b. Examination
c. Evaluation
d. Tekscan –T-Scan/3D airway modeling
e. Impressions/Facial/Intraoral/Model/ photographs — up load to Dr. Dave Singh
f. Deliver to lab for models to be available the morning of day two
i. Myotronics
ii. 3-D Scanner
iii. TENSing
g. Radiographs
h. Differential Diagnosis
4. Dr. Chapman/Dr. Preble—Review dental and neuromusculoskeletal findings via conference
a. AO Transdermal Atlas Positioning
b. Therapeutic Recovery
c. Post procedural radiographs
d. TENSing
5. Dr. Preble—Bite Registration (Part one)
Day Two:
1. Dr. Chapman—
a. Re-Evaluation, radiographs if needed
b. Repeat TAP if needed
c. Post Radiographs if corrected
2. Dr. Preble—Re-evaluate and provide patients with impression material bites for AO radiographic analysis; make temporary bite material for sleep test.
3. Dr. Chapman — Post check
4. Dr. Preble — Post check
Day Three:
1. Specialized craniospinal and craniofacial therapy—Two hours
Day Four:
1. Dr. Chapman—
a. Re-Evaluation
b. AO Transdermal Atlas Positioning
c. Post procedural radiographs with and without impression material
d. Matscan/T-Scan
e. 3D Body Scan
The above process may need to be repeated, refined to achieve complete and stable alignment of the atlas/axis and and the jaw and bite simultaneously. For when these structures are optimally placed, and stabilized, the entire body comes into greater functional harmony. The neuro-musculo-skeletal system is optimized and balanced. The neuro-cardio-respiratory system is also optimized. These are the root systems of the body, and they are entirely enmeshed functionally and anatomically. Occlusal support then not only rehabilitates the TMJ’s, but serves as a proprioceptive stabilizer for the entire body. The relationships of these systems is well documented and vastly described in the chiropractic, dental and medical literature. Thus, the AO procedure and occlusal therapy can optimize these complex, coordinated systems and resolve complicated health problems at a causative level.
Dental treatments for TMD, or any occlusion altering dental procedure should always involve (at a minimum) a consultation/examination from with a board certified Atlas Orthogonist who specializes in the T.A.P. procedures, and preferably one who is aptly educated and experienced in dealing with malocclusion. At the very least, I cannot over emphasize the importance of having a dependable scientific analysis of the alignment of the head, atlas and axis prior to TMD therapy by a Atlas Orthogonist or NUCCA doctor. This analysis should consist of at least a complete history, special physical examination, specialized x-rays or a CT scan called a CBCT, or cone-beam CT.
How will your dentist respond to the idea of atlas orthogonal therapy? It’s hard to say–sometimes we just have to find a new dentist… but the idea of a properly aligned atlas is not new to the dental profession. Research was done by dental researchers in the 1940’s, on the importance of the alignment of atlas and axis and it’s relationship to the jaw. I have posted a few of their original discoveries into the body of this article.
Success where others have treatments have failed:
Here at the Chapman Clinic for Spinal and Craniofacial Epigenetics, we have developed a multidisciplinary protocols in partnership with leading dentists and dental researchers, and have been implementing this protocol with great success. Part of this process included the formation of the website www.spinalepigenetics.com which is still in a state of development.
The reader should, by now, hopefully understand that our discussion of TMD, its diagnosis and subsequent treatment as presented here in this article is oriented towards the perspective that TMD develops from deeper pathologies, such as: Atlas Subluxation and Malocclusion.
In a paper entitled Dental Distress Syndrome, http://www.icnr.com/DentalDistressSyndrome/DentalDistressSyndrome.html Dr. A. C. Fonder, a great dental researcher describes the role of the Atlas and Axis (C1 and C2) in malocclusion and TMD, and lays the foundation for understanding the deeper problem which gives rise to malocclusion—which of course also provides a basis for understanding the pathology of TMD. Importantly, he also emphasizes the role that poor bite posture (which is essentially—malocclusion) plays in important role in the misaligning forces of the Occiput, C1 and C2—this is another topic—and it is a clue as to why some patients who have had their atlases realigned, have trouble keeping them in place!
I am posting a few important excerpts from his research below because it will enhance the readers understanding of the dentists’ perspective on the atlas and axis, and also should help enhance the upper cervical chirpractor’s perspective on the importance of the jaw:
THE NET-NET: WE NEED TO WORK TOGETHER!
“Mandibular Function”
According to Dr. Fonder: “To better understand how the dental system can effect distant bodily alterations in disease and health processes, we must consider the 68 pairs of muscles above and below the mandible. Together these 136 muscles determine head, cervical, shoulder and jaw posturization during all of life’s functional processes. Our Dental Research Group of Chicago began studying the functional movements of the mandible during the 1940’s.”
“This research shed new light on mandibular and condylar movements.29 A student of physics and engineering, Casey Guzay, put our findings into a sophisticated series of drawings entitled, The Quadrant Theorem. As determined, the muscle controlled pivotal axis of the mandible occurs at the dens between the atlas and axis vertebrae. Therefore, the mandibular dysfunction effects a disturbing posturing of C1 and C2. These vertebrae are intimately related to spinal and head posturing.” [emphasis added]
“Posture”
The malposturing of C1 and C2, through the dental malocclusion and the resultant mandibular dysfunctioning, torques the dura mater because of the frontal and dorsal attachments to C1, C2 and C3.
[Authors Note: The dura mater is a neurological connective tissue that is intimate to most of the axial skeleton. It lines the inside of the skull cavity, surrounds the brain, anchors to the foreman magnum (big hole at bottom of skull) attaches to Atlas and Axis, lines the canal of the spine surouding the cord and all spinal nerve roots, extending down to the tip of the tailbone where it “blends” or fuses with the coccygeal periosteum”.]
Torquing of the dura causes:
“Cervical Vertebrae”
“Why is the malposturing of C1 through C4 so critical?”
This mal-posturing appears to be one of the most important but most often overlooked aspects of the sequelae of mandibular dysfunction.
We gain a better understanding of the complex interaction between the dental occlusion, TMJ kinematics, and cervical function with an overview of the structures involved.
OVERVIEW: [parts a-e are a bit technical, and can be skipped if it gives you a headache, but it may be useful for some readers, so I’m putting it in the excerpt]
This research has been replicated by the Russian, Japanese, German, Canadian, American and other individual medical and dental scientists, dental groups and medico-dental research teams. The Japanese medico-dental research team of fifteen specialists treated over 6,000 patients who had not responded to conventional medical care. (Dr. Maehara, the group leader, says that his success rate is 90% when proper dental support is provided.) These cases included Parkinson, epilepsy and all of the above.
At Chapman Neurological Spine Institute, under the precision standard of care of the Atlas Orthogonal procedure, and frequently in conjunction with epigenetic dentists certified in a specific type of dental appliance called the DNA appliance, TMD sufferers often find significant and lasting relief.
My clinical protocols, which included multidisciplinary resources, have resolved TMD and its associated syndromes for hundreds of patients.
TMJ disorders should be assessed in the context of the entire head and neck region, and therefore may be viewed clinically as “a side-effect of a structural dysfunction stemming from the head and neck bite mislalignment“. So, TMD can be addressed effectively by addressing an underlying imbalance.
Essentially, what I have found is: TMD treatments utilizing corrective orthogonal protocols as a core corrective procedure have been highly successful. Another thing I have observed is: when the patients head and neck are restored to a normal aligned position through the AO procedure, this restoration significantly enhances the patient’s TMD dental protocols and treatment, and, in a high number of cases, can entirely resolve the syndrome within several weeks of the AO procedure.
If you are dealing with a TMJ issue or jaw pain presently, and whether you are working with a dentist or not, I advise you to come in for an examination/consultation. I lecture and present Atlas Orthogonal procedures to the epigenetic dentists, and more are learning and incorporating our procedures into their occlusion therapies. I also present the malocclusion complexities to the upper cervical specialiNot all dental specialist are oriented towards combining their therapy with AO—but there is a growing number of AO
Telephone consultations are available.
Doctor Christopher Chapman is a graduate of Palmer College of Chiropractic and is a Board Certified Chiropractic Physician. He is Board Certified in the Atlas Orthogonal Procedure. He serves as Adjunct Faculty – Palmer College of Chiropractic, Davenport, IA. and is an instructor for the BYU Internship Program for pre-medical, pre-chiropractic, pre-dental undergraduate students. He serves as Multidisciplinary Chair for the Prestigious Sweat Institute in Atlanta, GA. He is a certified instructor for the basic four modules for the Atlas Orthogonal Certification Program. He lectures nationally to a multidisciplinary audience of dentists, chiropractors and medical doctors on the subject of the atlas subluxation complex, the biomechanical effect atlas subluxation has on the craniofacial system, sleep and TMD. He co-teaches a course on co-management of malocclusion and atlas subluxation in a clinical setting. He has lectured for Biomodeling Solutions, The Sweat Institute, Arrowhead Laboratories, and has been a regular guest on A healthier Your Radio, and national health radio program. He is a regular presenter for Biomodeling Solutions Webinar Series and has presented original research and material on the combined morbidities of atlas subluxation and malocclusion. He is a current member of the UCPA and the ICA.
Presently, Dr. Chapman directs the only clinic in the United States that has a neuromuscular dentist certified in the DNA appliance protocols to provide occlusal support for the reduction of the Atlas Subluxation.
Dr. Chapman’s articles appear in the NUCCA Upper Cervical Monograph, text books on The Atlas Vertebral Subluxation Complex, The School of Natural Healing news letter and most recently published an article on the combined affect of Atlas Orthogonal adjustment and a biomimetic oral appliance in the Annal of Vertebral Subluxation Research.
The Chapman Clinic for Spinal Epigenetics is a registered internship facility with Brigham Young University. Candidates for this Internship program have gone on to study chiropractic, hoping to eventually specialize in the Orthogonal based upper cervical chiropractic techniques. Currently Dr. Chapman is writing a book describing the essential role that posture plays in human health.

Dr. Chris Chapman, DC, BCAO
Chapman Clinic for Spinal Epigenetics
Chapman Clinic for Spinal Epigenetics
Dental based treatment for TMJ Dysfunction and malocclusion may be enhanced by combining therapy with Atlas Aligning Chiropractic procedures known as Atlas Orthogonal. Essentially, getting one’s head on straight through specialized atlas postitioning technology can make all the difference in whether the TMJ treatment is successful or a failure.
The Atlas Orthogonal (AO) procedure can restore the essential balance and positioning of the head, neck and back–a vital part of jaw function.
Malpositions of the head and neck are often associated with a common jaw disorder called Temporomandibular Joint (TMJ) Dysfunction, or TMD. TMD is also known as TMJ Syndrome. Patients that present to a specialized dentist for TMJ treatment are often not diagnosed for craniospinal dysfunction, hence, with only half the correct diagnosis, only a partial therapeutic program is recommended.
UNDERSTANDING THE TEMPOROMANDIBULAR JOINT (TMJ):
The jaw joint is way more than a “functional hinge” joint—it is more accurately described as being suspended and “docked” in the TMJ space rather than being anchored there—much the way the boat occupies the space in a slip. In the illustration below, you can see that when the mouth is open, the head of the condyle moves down and forward. The jaw or mandible is positioned and moved by 68 pairs of muscles of the head, neck, face and shoulders, and, unlike the vast majority of other joints of the body—which remain in their location during joint range of motion—the jaw joints are compensating joints to some extent, and glide into and out of the TMJ space based on its’ natural functional movement. Therapeutically, I have found that it helps to view the tempromadibular joints as more of a biomechanical “reference point”, rather than a fixed pivot or anchor point. TMJ function, it’s neurology and ability to compensate can be a complex clinical condition.
I cannot underscore the importance of having a multidisciplinary understanding of the mandibles sophisticated behavior patterns and it’s relationships with other structures such as the atlas and the axis vertebraes (C1 and C2), as well as the 68 pairs of muscles that move and position the jaw—-this knowledge is essential when treating complex TMD.T

The good news is: Although the TMJ is very complex, it does have a simple, identifiable “axis of movement” — and that axis of motion is not in the jaw joint itself! Rather, the axis of angular rotation of the mandible is around a very important structure in cervical spine, namely, C2 vertebrae, also known as the Axis (red line). The upward jutting structure on the Axis vertebrae around which the jaw “functionally” pivots on it’s several axes is called: the “dens”. The name “dens” provides an important clue, for in Latin, dens means: “tooth”!! So, the functional axis of the jaw, and hence the dynamic pivot of occlusion, takes place around the only part of the human spine which anatomists—centuries ago I might add—dubbed the “Tooth of the Spine”… Amazing, isn’t it!?

Open Mouth Projection showing the odontoid process
TMD Syndrome may occur when the normal functional “positions” of the jaw joints shift into irregular positions during movement and use. An uneven “grinding” or “wearing” use-pattern will likely develop, and is measurable through specialized instrumentation. This abnormal use-pattern and positioning can cause a significant amount of pain and inflammation–it can even cause tooth wear patterns, and may make chewing, sleeping, speaking and even breathing difficult.

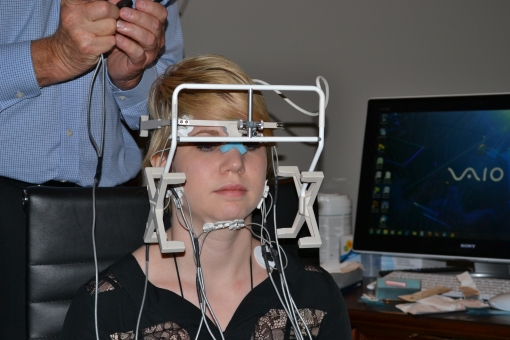
Surface EMG, electronic jaw tracking and TENSing assist in finding ideal jaw position
It is sort of like herding cats…
The Atlas Orthogonal (AO) treatment is a corrective cervical spine alignment procedure performed by Board Certified Atlas Orthogonists (BCAO) chiropractic physicians.
The AO specialist utilizes 3-dimensional images (via CT or X-ray) to locate and identify abnormal malpositions of the skull, the atlas, the axis and the other 5 cervical vertebraes. Once the exact malposition has been mapped out in 3-D space, a biomechanical analysis protocol is used to derive a mathematically formulated vector.

Specialized software is used to derive atlas positioning trajectory

A patient in the side lying position prepared to receive the painless Transdermal Atlas Positioning Procedure
A Sample of our Multidisciplinary Schedule on Week One
Day One:
1. Paperwork:
a. General Medical
b. Dental
2. Dr. Chapman –
a. History
b. Examination; CROM; vitals
c. Evaluation
d. Tekscan –Matscan
e. Radiographs/Cone Beam CT
f. Differential Diagnosis
3. Dr. Preble –
a. History
b. Examination
c. Evaluation
d. Tekscan –T-Scan/3D airway modeling
e. Impressions/Facial/Intraoral/Model/ photographs — up load to Dr. Dave Singh
f. Deliver to lab for models to be available the morning of day two
i. Myotronics
ii. 3-D Scanner
iii. TENSing
g. Radiographs
h. Differential Diagnosis
4. Dr. Chapman/Dr. Preble—Review dental and neuromusculoskeletal findings via conference
a. AO Transdermal Atlas Positioning
b. Therapeutic Recovery
c. Post procedural radiographs
d. TENSing
5. Dr. Preble—Bite Registration (Part one)
Day Two:
1. Dr. Chapman—
a. Re-Evaluation, radiographs if needed
b. Repeat TAP if needed
c. Post Radiographs if corrected
2. Dr. Preble—Re-evaluate and provide patients with impression material bites for AO radiographic analysis; make temporary bite material for sleep test.
3. Dr. Chapman — Post check
4. Dr. Preble — Post check
Day Three:
1. Specialized craniospinal and craniofacial therapy—Two hours
Day Four:
1. Dr. Chapman—
a. Re-Evaluation
b. AO Transdermal Atlas Positioning
c. Post procedural radiographs with and without impression material
d. Matscan/T-Scan
e. 3D Body Scan
The above process may need to be repeated, refined to achieve complete and stable alignment of the atlas/axis and and the jaw and bite simultaneously. For when these structures are optimally placed, and stabilized, the entire body comes into greater functional harmony. The neuro-musculo-skeletal system is optimized and balanced. The neuro-cardio-respiratory system is also optimized. These are the root systems of the body, and they are entirely enmeshed functionally and anatomically. Occlusal support then not only rehabilitates the TMJ’s, but serves as a proprioceptive stabilizer for the entire body. The relationships of these systems is well documented and vastly described in the chiropractic, dental and medical literature. Thus, the AO procedure and occlusal therapy can optimize these complex, coordinated systems and resolve complicated health problems at a causative level.
Dental treatments for TMD, or any occlusion altering dental procedure should always involve (at a minimum) a consultation/examination from with a board certified Atlas Orthogonist who specializes in the T.A.P. procedures, and preferably one who is aptly educated and experienced in dealing with malocclusion. At the very least, I cannot over emphasize the importance of having a dependable scientific analysis of the alignment of the head, atlas and axis prior to TMD therapy by a Atlas Orthogonist or NUCCA doctor. This analysis should consist of at least a complete history, special physical examination, specialized x-rays or a CT scan called a CBCT, or cone-beam CT.
How will your dentist respond to the idea of atlas orthogonal therapy? It’s hard to say–sometimes we just have to find a new dentist… but the idea of a properly aligned atlas is not new to the dental profession. Research was done by dental researchers in the 1940’s, on the importance of the alignment of atlas and axis and it’s relationship to the jaw. I have posted a few of their original discoveries into the body of this article.
Success where others have treatments have failed:
Here at the Chapman Clinic for Spinal and Craniofacial Epigenetics, we have developed a multidisciplinary protocols in partnership with leading dentists and dental researchers, and have been implementing this protocol with great success. Part of this process included the formation of the website www.spinalepigenetics.com which is still in a state of development.
The reader should, by now, hopefully understand that our discussion of TMD, its diagnosis and subsequent treatment as presented here in this article is oriented towards the perspective that TMD develops from deeper pathologies, such as: Atlas Subluxation and Malocclusion.
In a paper entitled Dental Distress Syndrome, http://www.icnr.com/DentalDistressSyndrome/DentalDistressSyndrome.html Dr. A. C. Fonder, a great dental researcher describes the role of the Atlas and Axis (C1 and C2) in malocclusion and TMD, and lays the foundation for understanding the deeper problem which gives rise to malocclusion—which of course also provides a basis for understanding the pathology of TMD. Importantly, he also emphasizes the role that poor bite posture (which is essentially—malocclusion) plays in important role in the misaligning forces of the Occiput, C1 and C2—this is another topic—and it is a clue as to why some patients who have had their atlases realigned, have trouble keeping them in place!
I am posting a few important excerpts from his research below because it will enhance the readers understanding of the dentists’ perspective on the atlas and axis, and also should help enhance the upper cervical chirpractor’s perspective on the importance of the jaw:
THE NET-NET: WE NEED TO WORK TOGETHER!
“Mandibular Function”
According to Dr. Fonder: “To better understand how the dental system can effect distant bodily alterations in disease and health processes, we must consider the 68 pairs of muscles above and below the mandible. Together these 136 muscles determine head, cervical, shoulder and jaw posturization during all of life’s functional processes. Our Dental Research Group of Chicago began studying the functional movements of the mandible during the 1940’s.”
“This research shed new light on mandibular and condylar movements.29 A student of physics and engineering, Casey Guzay, put our findings into a sophisticated series of drawings entitled, The Quadrant Theorem. As determined, the muscle controlled pivotal axis of the mandible occurs at the dens between the atlas and axis vertebrae. Therefore, the mandibular dysfunction effects a disturbing posturing of C1 and C2. These vertebrae are intimately related to spinal and head posturing.” [emphasis added]
“Posture”
The malposturing of C1 and C2, through the dental malocclusion and the resultant mandibular dysfunctioning, torques the dura mater because of the frontal and dorsal attachments to C1, C2 and C3.
[Authors Note: The dura mater is a neurological connective tissue that is intimate to most of the axial skeleton. It lines the inside of the skull cavity, surrounds the brain, anchors to the foreman magnum (big hole at bottom of skull) attaches to Atlas and Axis, lines the canal of the spine surouding the cord and all spinal nerve roots, extending down to the tip of the tailbone where it “blends” or fuses with the coccygeal periosteum”.]
Torquing of the dura causes:
- 1. scoliosis,
- 2. cervical hypolordosis (military neck),
- 3. thoracic hyperkyphosis (hump back),
- 4. excessive lumbar lordosis (sway back),
- rotation of the pelvis causing uneven leg length,
- 6. uneven shoulder height, etc.
- 7. it also aids in creating head tilt through the dura’s attachment around the foramen magnum.
- The cranial bones, because of their multiple attachments to the dura can also be malpostured through this torquing stress of the dura mater.
“Cervical Vertebrae”
“Why is the malposturing of C1 through C4 so critical?”
This mal-posturing appears to be one of the most important but most often overlooked aspects of the sequelae of mandibular dysfunction.
We gain a better understanding of the complex interaction between the dental occlusion, TMJ kinematics, and cervical function with an overview of the structures involved.
OVERVIEW: [parts a-e are a bit technical, and can be skipped if it gives you a headache, but it may be useful for some readers, so I’m putting it in the excerpt]
- a. Rene Cailliet, Physical Medicine and Rehabilitation Director at U.S.C. states:
- b. Kapandji, in his classic text on spinal function states:
- c. Numerous investigators describe the effect of altered mandibular position on cranial posture:
- d. Concentrating on the cervical apophyseal joints, we observe the role of the mechanoreceptors that dominate the vestibular system in relation to the reflex regulation of static posture and gait.
- e. The cervical mechanoreceptors also have a potent effect on eye control, speech, and manual dexterity.
This research has been replicated by the Russian, Japanese, German, Canadian, American and other individual medical and dental scientists, dental groups and medico-dental research teams. The Japanese medico-dental research team of fifteen specialists treated over 6,000 patients who had not responded to conventional medical care. (Dr. Maehara, the group leader, says that his success rate is 90% when proper dental support is provided.) These cases included Parkinson, epilepsy and all of the above.
At Chapman Neurological Spine Institute, under the precision standard of care of the Atlas Orthogonal procedure, and frequently in conjunction with epigenetic dentists certified in a specific type of dental appliance called the DNA appliance, TMD sufferers often find significant and lasting relief.
My clinical protocols, which included multidisciplinary resources, have resolved TMD and its associated syndromes for hundreds of patients.
TMJ disorders should be assessed in the context of the entire head and neck region, and therefore may be viewed clinically as “a side-effect of a structural dysfunction stemming from the head and neck bite mislalignment“. So, TMD can be addressed effectively by addressing an underlying imbalance.
Essentially, what I have found is: TMD treatments utilizing corrective orthogonal protocols as a core corrective procedure have been highly successful. Another thing I have observed is: when the patients head and neck are restored to a normal aligned position through the AO procedure, this restoration significantly enhances the patient’s TMD dental protocols and treatment, and, in a high number of cases, can entirely resolve the syndrome within several weeks of the AO procedure.
If you are dealing with a TMJ issue or jaw pain presently, and whether you are working with a dentist or not, I advise you to come in for an examination/consultation. I lecture and present Atlas Orthogonal procedures to the epigenetic dentists, and more are learning and incorporating our procedures into their occlusion therapies. I also present the malocclusion complexities to the upper cervical specialiNot all dental specialist are oriented towards combining their therapy with AO—but there is a growing number of AO
Telephone consultations are available.
Doctor Christopher Chapman is a graduate of Palmer College of Chiropractic and is a Board Certified Chiropractic Physician. He is Board Certified in the Atlas Orthogonal Procedure. He serves as Adjunct Faculty – Palmer College of Chiropractic, Davenport, IA. and is an instructor for the BYU Internship Program for pre-medical, pre-chiropractic, pre-dental undergraduate students. He serves as Multidisciplinary Chair for the Prestigious Sweat Institute in Atlanta, GA. He is a certified instructor for the basic four modules for the Atlas Orthogonal Certification Program. He lectures nationally to a multidisciplinary audience of dentists, chiropractors and medical doctors on the subject of the atlas subluxation complex, the biomechanical effect atlas subluxation has on the craniofacial system, sleep and TMD. He co-teaches a course on co-management of malocclusion and atlas subluxation in a clinical setting. He has lectured for Biomodeling Solutions, The Sweat Institute, Arrowhead Laboratories, and has been a regular guest on A healthier Your Radio, and national health radio program. He is a regular presenter for Biomodeling Solutions Webinar Series and has presented original research and material on the combined morbidities of atlas subluxation and malocclusion. He is a current member of the UCPA and the ICA.
Presently, Dr. Chapman directs the only clinic in the United States that has a neuromuscular dentist certified in the DNA appliance protocols to provide occlusal support for the reduction of the Atlas Subluxation.
Dr. Chapman’s articles appear in the NUCCA Upper Cervical Monograph, text books on The Atlas Vertebral Subluxation Complex, The School of Natural Healing news letter and most recently published an article on the combined affect of Atlas Orthogonal adjustment and a biomimetic oral appliance in the Annal of Vertebral Subluxation Research.
The Chapman Clinic for Spinal Epigenetics is a registered internship facility with Brigham Young University. Candidates for this Internship program have gone on to study chiropractic, hoping to eventually specialize in the Orthogonal based upper cervical chiropractic techniques. Currently Dr. Chapman is writing a book describing the essential role that posture plays in human health.
Anyone who has looked at our NUCCA Spinal Centers Facebook page knows that we have a strong interest in helping families obtain better health—and lately, our pediatric focus has increased significantly. I want to talk about the various symptoms and signs that parents or care-givers can look for in their babies to keep them misalignment free.
To begin with, anyone who has raised a child into adulthood knows what a tremendous and ongoing project that is—our children don’t truly appreciate it until they have their own, right?
There are so many wonderful blessings associated with the raising of children—and then with grandchildren…. But I want to talk about some of the health challenges that effect our littlest members of our community—our babies and small children.
This is where it can be very challenging and stressful for young families. I remember my oldest child—he had a very long and traumatic delivery.
After a long and stressful delivery process, he seemed to be OK for several months, health-wise, until…… he started developing ear infections and breathing problems like pneumonia and asthma. And nothing concerns a parent more to see their child in respiratory distress, struggling to draw in breath.
In the case of my oldest son, those problems evolved into pneumonia, recurrent ear infections and chronic bronchitis—and, of course that led to copious amounts of that pink, bubble-gum flavored elixir——–Amoxicillin. I don’t think it really helped, for if it had, well… we wouldn’t have been filling a prescription 2X a month for months on end.
We didn’t know what to do—he was our first, and we were cutting our teeth on him before he even started cutting his. We turned, as millions do, to our pediatrician. I did not know about upper cervical chiropractic care, what a subluxation was or even herbs.
Well, we all survived, and our young children survived, each with their own individual health challenges until one day in early 1992, I was in a car accident… Well, it seems that every accident that I have had, changes my life in some way. This particular accident placed me in a chiropractor’s office in search of treatment for my migraines, and those visits with my doctor led to “the epiphany”—rather the calling to go back to school and get my doctorate. Had I not had that accident, I am not sure I would be here right now discussing these excellent health solutions for your young infants.
So let’s talk about what to look for in our babies. By babies, I am referring to little infants, usually under two years old. First, traumatic birth processes are something to be concerned with. A traumatic birth process raises the probability that the infant suffered mechanical forces which caused a problem, or set the stage for health problems that will show up later.
Trauma of any kind can cause a persistent misalignment between their small head and neck, but birth is often the “first trauma”.
That “persistent misalignment” is referred to as a subluxation. Frequently, but not always does excessive birth trauma result in subluxation, however, more often than not—IT DOES. I will be presenting some signs of what to look out for in just a moment, but first I want to define what a subluxation is:
Subluxation: a persistent misalignment, or malposition of the head as it joins the top ring shaped bone of the neck which causes interference in the normal function of the nervous system and other normal functions such as blood flow, cerebrospinal fluid flow, etc. Thus, there are signs and symptoms associated with subluxation. Think of it as though the head were a lid on a mason jar, and the lid is threaded on the jar crookedly and tightened down slightly askew. The lid (head) is misaligned on the jar (neck).
BIRTH TRAUMA CAUSES:
1. Intra-uterine Difficulties
2. Delivery Canal Difficulties
3. Mechanical Delivery Distress
a. Forceps
b. Abnormal Presentations
c. Cesarean Deliveries
SYMPTOMS AND SIGNS: (a partial list)
1. Ear infections—acute otitis media, or serous otitis media
2. Eye infections—blocked tear duct, chronic conjunctivitis, or other reoccurring infections of the eyes, ears, nose or throat
3. Colic
4. Respiratory infections
5. Asthma
6. Not sleeping well
7. Failure to thrive
8. Grumpy, irritable
9. Excessive crying
10. Antibiotic use of any kind
What physical signs to look for in infants: (a partial list)
1. A head that remains persistently bent or turned in one direction
2. A difference in active movement patterns between right and left side arms and legs
3. A gentle tendency to bend their body to one side over another
4. Greater difficulty in nursing – one position is more difficult than the other.
5. Odd sleeping positions: head hanging off bed, stomach sleeping, arched to the side, or arched-back
6. Abnormal function of the eyes, such as a lazy eye, or converging eye
7. Misshapen cranial bones
8. Non-genetic Asymmetry in facial features
9. Down Syndrome
10. Asymmetric hair wear patterns
SYMPTOMS CHILDREN:
1. Autism
2. ADD
3. ADHD
4. Seizures: petit mal, or more tonic clonic variety
5. Bed wetting
6. Chronic Infections,
a. ear,
b. eye,
c. respiratory,
d. skin
7. Asthma
8. Anxiety
9. Digestive Disorders (of course, this can also be diet)
The world doesn’t seem to be child-proof—I think that is why so many parents are bringing their children in to have them evaluated early on, when fresh misalignments first begin to interfere with lives. Our goal is to get the knowledge out there to the general populace in hopes that many developmental problems can be nipped in the bud early on. A lot of suffering and searching can be circumvented through early detection and correction.
CASES:
I have documented hundreds of these cases in my practice over the years. More recently, I have begun filming the examination and the correction procedure and placing some of those on the web.
If you want to take a look at those cases, type in “nucca spinal centers facebook” on your web brouser. You will likely get to our facebook page where you can see live videos of the correction being performed on our little patients. It really is quite a fantastic process and procedure. It’s simple.
Of the symptoms I have mentioned above, most of the time, a simple, straight forward NUCCA correction solves the problem. Other times there are other challenges that need to be addressed. We take those on a case by case basis.
We aren’t encouraging parents to dump their pediatricians—on the contrary, tell your pediatrician what you are doing—if you feel comfortable with it. Most of them will “glass-over” when you do, but some will listen and get on board with you. They serve a purpose, and as health professionals, it is nice to work together, even if we do nothing more than provide counterpoint arguments to each other’s perspective.
Most of the pediatric solutions to the above problems will result in a trip to the pharmacy for antibiotics or some other medication – or, a surgical procedure like myringotomy (tubes and incision), or, in the case of some of the postural signs that I have shared with you—they will be shrugged off as irrelevant. However, as I have pointed out in the section on what to look for—they are important and should not be dismissed.
Here is the good news: In my practice, with my protocols, there is a dependable analysis and examination which detects and corrects the infant subluxation. Most of the time, if we detect the subluxation before the age of three, we don’t need X-rays. Rarely will I take them on infants.
However, after 3-years of age, it is almost impossible to correct them without X-rays. So there is this wonderful window of opportunity to detect and correct at an early age.
And that’s what our Balanced Baby program is all about— Detection and Correction.
I BELIEVE THAT EVERY BABY SHOULD BE CHECKED FOR SUBLUXATION! So many problems can be prevented.
“As the twig is bent, doth grow the tree”
(801) 655-1801
To begin with, anyone who has raised a child into adulthood knows what a tremendous and ongoing project that is—our children don’t truly appreciate it until they have their own, right?
There are so many wonderful blessings associated with the raising of children—and then with grandchildren…. But I want to talk about some of the health challenges that effect our littlest members of our community—our babies and small children.
This is where it can be very challenging and stressful for young families. I remember my oldest child—he had a very long and traumatic delivery.
After a long and stressful delivery process, he seemed to be OK for several months, health-wise, until…… he started developing ear infections and breathing problems like pneumonia and asthma. And nothing concerns a parent more to see their child in respiratory distress, struggling to draw in breath.
In the case of my oldest son, those problems evolved into pneumonia, recurrent ear infections and chronic bronchitis—and, of course that led to copious amounts of that pink, bubble-gum flavored elixir——–Amoxicillin. I don’t think it really helped, for if it had, well… we wouldn’t have been filling a prescription 2X a month for months on end.
We didn’t know what to do—he was our first, and we were cutting our teeth on him before he even started cutting his. We turned, as millions do, to our pediatrician. I did not know about upper cervical chiropractic care, what a subluxation was or even herbs.
Well, we all survived, and our young children survived, each with their own individual health challenges until one day in early 1992, I was in a car accident… Well, it seems that every accident that I have had, changes my life in some way. This particular accident placed me in a chiropractor’s office in search of treatment for my migraines, and those visits with my doctor led to “the epiphany”—rather the calling to go back to school and get my doctorate. Had I not had that accident, I am not sure I would be here right now discussing these excellent health solutions for your young infants.
So let’s talk about what to look for in our babies. By babies, I am referring to little infants, usually under two years old. First, traumatic birth processes are something to be concerned with. A traumatic birth process raises the probability that the infant suffered mechanical forces which caused a problem, or set the stage for health problems that will show up later.
Trauma of any kind can cause a persistent misalignment between their small head and neck, but birth is often the “first trauma”.
That “persistent misalignment” is referred to as a subluxation. Frequently, but not always does excessive birth trauma result in subluxation, however, more often than not—IT DOES. I will be presenting some signs of what to look out for in just a moment, but first I want to define what a subluxation is:
Subluxation: a persistent misalignment, or malposition of the head as it joins the top ring shaped bone of the neck which causes interference in the normal function of the nervous system and other normal functions such as blood flow, cerebrospinal fluid flow, etc. Thus, there are signs and symptoms associated with subluxation. Think of it as though the head were a lid on a mason jar, and the lid is threaded on the jar crookedly and tightened down slightly askew. The lid (head) is misaligned on the jar (neck).
BIRTH TRAUMA CAUSES:
1. Intra-uterine Difficulties
2. Delivery Canal Difficulties
3. Mechanical Delivery Distress
a. Forceps
b. Abnormal Presentations
c. Cesarean Deliveries
SYMPTOMS AND SIGNS: (a partial list)
1. Ear infections—acute otitis media, or serous otitis media
2. Eye infections—blocked tear duct, chronic conjunctivitis, or other reoccurring infections of the eyes, ears, nose or throat
3. Colic
4. Respiratory infections
5. Asthma
6. Not sleeping well
7. Failure to thrive
8. Grumpy, irritable
9. Excessive crying
10. Antibiotic use of any kind
What physical signs to look for in infants: (a partial list)
1. A head that remains persistently bent or turned in one direction
2. A difference in active movement patterns between right and left side arms and legs
3. A gentle tendency to bend their body to one side over another
4. Greater difficulty in nursing – one position is more difficult than the other.
5. Odd sleeping positions: head hanging off bed, stomach sleeping, arched to the side, or arched-back
6. Abnormal function of the eyes, such as a lazy eye, or converging eye
7. Misshapen cranial bones
8. Non-genetic Asymmetry in facial features
9. Down Syndrome
10. Asymmetric hair wear patterns
SYMPTOMS CHILDREN:
1. Autism
2. ADD
3. ADHD
4. Seizures: petit mal, or more tonic clonic variety
5. Bed wetting
6. Chronic Infections,
a. ear,
b. eye,
c. respiratory,
d. skin
7. Asthma
8. Anxiety
9. Digestive Disorders (of course, this can also be diet)
The world doesn’t seem to be child-proof—I think that is why so many parents are bringing their children in to have them evaluated early on, when fresh misalignments first begin to interfere with lives. Our goal is to get the knowledge out there to the general populace in hopes that many developmental problems can be nipped in the bud early on. A lot of suffering and searching can be circumvented through early detection and correction.
CASES:
I have documented hundreds of these cases in my practice over the years. More recently, I have begun filming the examination and the correction procedure and placing some of those on the web.
If you want to take a look at those cases, type in “nucca spinal centers facebook” on your web brouser. You will likely get to our facebook page where you can see live videos of the correction being performed on our little patients. It really is quite a fantastic process and procedure. It’s simple.
Of the symptoms I have mentioned above, most of the time, a simple, straight forward NUCCA correction solves the problem. Other times there are other challenges that need to be addressed. We take those on a case by case basis.
We aren’t encouraging parents to dump their pediatricians—on the contrary, tell your pediatrician what you are doing—if you feel comfortable with it. Most of them will “glass-over” when you do, but some will listen and get on board with you. They serve a purpose, and as health professionals, it is nice to work together, even if we do nothing more than provide counterpoint arguments to each other’s perspective.
Most of the pediatric solutions to the above problems will result in a trip to the pharmacy for antibiotics or some other medication – or, a surgical procedure like myringotomy (tubes and incision), or, in the case of some of the postural signs that I have shared with you—they will be shrugged off as irrelevant. However, as I have pointed out in the section on what to look for—they are important and should not be dismissed.
Here is the good news: In my practice, with my protocols, there is a dependable analysis and examination which detects and corrects the infant subluxation. Most of the time, if we detect the subluxation before the age of three, we don’t need X-rays. Rarely will I take them on infants.
However, after 3-years of age, it is almost impossible to correct them without X-rays. So there is this wonderful window of opportunity to detect and correct at an early age.
And that’s what our Balanced Baby program is all about— Detection and Correction.
I BELIEVE THAT EVERY BABY SHOULD BE CHECKED FOR SUBLUXATION! So many problems can be prevented.
“As the twig is bent, doth grow the tree”
(801) 655-1801
The following link shows a brief video of a 3-month-old infant who is a candidate for the NUCCA corrective procedure. She has noticeable body arching, a blocked tear duct and acute otitis media. My experience has shown that these are symptoms that can be related to a traumatic birth, which she did experience. To see both parts of the video, cut and paste the link in your browser.
PART I
http://www.facebook.com/video/video.php?v=1612258939698&ref=mf
Following our examination, we then corrected little Kaitlyn. Follow the links to see the pre/post videos and to view the corrective procedure.
PART II
http://www.facebook.com/video/video.php?v=1616679890219&ref=mf
PART I
http://www.facebook.com/video/video.php?v=1612258939698&ref=mf
Following our examination, we then corrected little Kaitlyn. Follow the links to see the pre/post videos and to view the corrective procedure.
PART II
http://www.facebook.com/video/video.php?v=1616679890219&ref=mf
Have you ever wished that you could turn back the hands of time?
Imagine stepping out side after a cleansing rain storm and seeing an up-side-down rainbow, resting like an immense singing bowl on the Earth, rather than an arch above it. You would know that something was seriously wrong— But we know that this phenomenon could never happen because of the nature of the laws of physics that govern our atmosphere. And yet, there is a common, almost casual acceptance of the reversal of one of our most natural arches—the arch of our neck.
What is normal?
When looking at the neck through the “eyes” of an X-ray machine, a graceful, lordotic curve is “normal”. That means that the convexity of the arch is to the front as shown below on the right. This is called a lordosis. Lordosis is the “normal” position for the neck and the low back. However, after certain structural stressors, many people—including children and the elderly—have a reversal of this normal lordosis. I will discuss the adverse symptoms of a reversed, abnormal curve.


Before Curve Restoration After Curve Restoration
But first, let us look at some of the causes:
The most common cause of a reversed curve of the neck is from accidents and injuries, like falls, sporting injuries and car accidents—even very low speed crashes of less than 5 MPH where there is no damage to the vehicle. These traumatic events can cause damage to the connective tissues that hold the neck and the head within proper boundaries, adversely effecting nerves, blood vessels, lymphatic drainage and the muscles of the head, neck, upper back and jaw. The muscles can remain in a stressed position, which can become the CAUSE of many of the symptoms that originate from this area. Symptoms can be diverse—- with Migraines, Vertigo, TMJ disorders and Face and Neck Pain being just the tip of the iceberg…
What is a very common finding in the cervical spine, following head and neck trauma? The “Lateral” view seen above on the left was taken before the specific upper cervical correction was performed, but shortly after a minor motor vehicle accident—this is the common finding! This otherwise healthy, fit patient had severe spasm of the neck muscles; resulting in a very painful condition we call Spasmodic Torticollis. This X-ray was taken four weeks following a “very minor” car accident wherein the patient slid side-ways into a curb. The damage to the car was minimal. Yet, the patient cannot even raise her head to the normal upright position because the spasms are so intense. The X-ray on the right shows a return of the normal curve. The GOOD NEWS is: These structures can very often be appropriately realigned and when they are, the body will began repairing and healing the injured areas.
The X-ray on the right is the corrected spinal curve, having returned to true normal lordosis following only 5 NUCCA treatments! There were no other modalities performed on this patient. I’ve seen hundreds, if not thousands of cervical curves restored with NUCCA and Atlas Orthogonal (AO). What’s hard for me to fathom, is that Emergency Departments around the country are missing the harm and potential problems that can arise from a reversed or straight neck. The stressed position of the neck as seen on the left is a common finding, and it is often trivialized or dismissed as “normal”. I can see this casual dismissal in some ways. for instance, this important finding is diminished as emergency room staff focus more on “life-threatening” immediate risk problems, and less on conditions and “findings” which might develop into long-term chronic health conditions—it’s simply not their job. Muscle relaxants may be prescribed, but my practical experience in dealing with thousands of patients “after-the-fact” is: taking relaxants will not restore the cervical curve. Further, if left uncorrected, this reversed curve can contribute to the many symptoms and syndromes that are linked to head and neck misalignments, like:
The most vulnerable area of the spine is where the head rests on the neck. The top bone (called the Atlas) is a small 2-ounce ring-shaped bone with 2 small divots on either side of the spinal cord called facets—these small joints support the full weight of the skull. The adult skull often weighs more than 13 pounds! Imagine—a bowling ball mass being supported by two golf tees! But don’t be fooled—even with what appears to be a “fragile design flaw” in our anatomy, it is quite hardy—except under certain traumatic conditions; then, it can become quite vulnerable to injuries. When this area is fundamentally disturbed through trauma, the head—–and the atlas upon which it rests, lose their normal healthy alignment with one another; the result is a distortion of the spine, the spinal cord and it’s supportive tissues. There is also the possibility of a disturbance of blood flow to and from the brain.
This head and atlas malposition then causes the supporting spinal muscles to contract irregularly in compensation, and will cause the entire spine to distort out-of-balance, thereby effecting the entire body. This upper cervical distortion will almost always result in a high or low hip, a “shortened leg” syndrome ( http://www.myshortleg.com/ ), and usually a high or low shoulder. Often the head will tilt slightly to one side or the other, and the abnormal contraction of the neck muscles will force the normal lordotic curve into a reversed or straightened position—this is COMMON, but not NORMAL. Specific upper cervical X-rays will reveal the misalignment in a multidimensional fashion.
The X-ray views taken following trauma in the Emergency Room, or a doctor’s office will perhaps reveal the reversed curve, but provide little information on what’s causing it or how to fix it.
In my 15 years of practice, I have seen many forms of “therapy” designed to “restore” the normal cervical curve. Some of them you would think were designed more as torture techniques borrowed from a mad scientist laboratory than sound medical restorative therapies. One of the most ludicrous is a technique that situates the back of the neck on a “fulcrum”, while heavy weights are suspended from the forehead using gravity to literally force the head into extension! Well, I can say with certainty: there IS a better way to restore a normal, lordotic neck curve. That way is to get right down to the cause and correct it.
CASE IN POINT:
The X-rays below were taken over a 16-month period. There were only 5 Atlas corrections made over that time period. The X-rays are of a 19-year-old female with a history of gradual onset of neck pain, which became suddenly severe 4 weeks following her sliding side-ways into a curb while traveling as a passenger in a moving vehicle. She estimated her speed to be under 10mph. The front wheel of the car was only “slightly damaged”, and she was quite sure that such a “small bump” could not have caused her severe neck spasms.


Pre-Correction 1st Post-Correction


At 4 Months At 12 Months
Notice in the first view how her head pitches downward due to cervical muscle spasms. The patient could not lift her head any higher than this due to muscle spasms. This is what Spasmodic Torticollis looks like from the side view on an X-ray.
The first “Post” view was taken immediately following the first upper cervical procedure, and you can actually see how the muscle spasms have diminished, allowing the head and neck to begin returning to a normal position. Four months later the head is making progress with only one intervening Orthogonal Atlas adjustment having been performed. Three more Atlas “Corrections” were given over the next 12 months. In the last view, the normal curve has been restored without using contraptions or force.
Gone is the neck pain, the migraines and jaw pain. Happy is the patient!
We may not have turned back the hands of time, but for this young lady who is now 23, we have effectively taken her out of the fast-lane towards spinal degeneration, and essentially saved her from many years of painful struggle.
If you, or someone you know suffers, perhaps that suffering is needless. Don’t wait—we’re here to help.
Authors Note: In the X-rays taken above, a duplication of the patient’s “hard palate angle” seen in the first Post Correction was used as a base line. The author is aware that, though not “on level” as is the measuring convention, it was important to maintain the initial sloped palate angle in order to accurately compare subsequent X-rays as raising up the angle would induce an artifactual increase in curve.
Bio: Doctor Christopher Chapman is a graduate of Palmer College of Chiropractic and is a Board Certified Chiropractic Physician. He practices exclusively the Atlas Orthogonal (AO) and NUCCA procedures in Provo, Utah using certified aligned X-ray equipment. He has published articles on the etiology of Atlas Subluxation, lectures nationally to a multidisciplinary audience of dentists, chiropractors and is pioneering orthogonal based spinal procedures in association with leading researchers in the field of Epigenetics. He is the Clinic Director for the Chapman Clinic for Spinal and Craniofacial Epigenetics and currently instructs and mentors Associate Doctors interested in perfecting the clinical application of the Atlas Orthogonal procedure. NUCCA Spinal Centers is an authorized internship facility associated with Brigham Young University. Interns from this program have gone on to study chiropractic, hoping to eventually specialize in the Orthogonal based upper cervical techniques. Telephone consultations are available by calling 801.655.1801.
Imagine stepping out side after a cleansing rain storm and seeing an up-side-down rainbow, resting like an immense singing bowl on the Earth, rather than an arch above it. You would know that something was seriously wrong— But we know that this phenomenon could never happen because of the nature of the laws of physics that govern our atmosphere. And yet, there is a common, almost casual acceptance of the reversal of one of our most natural arches—the arch of our neck.
What is normal?
When looking at the neck through the “eyes” of an X-ray machine, a graceful, lordotic curve is “normal”. That means that the convexity of the arch is to the front as shown below on the right. This is called a lordosis. Lordosis is the “normal” position for the neck and the low back. However, after certain structural stressors, many people—including children and the elderly—have a reversal of this normal lordosis. I will discuss the adverse symptoms of a reversed, abnormal curve.


Before Curve Restoration After Curve Restoration
But first, let us look at some of the causes:
The most common cause of a reversed curve of the neck is from accidents and injuries, like falls, sporting injuries and car accidents—even very low speed crashes of less than 5 MPH where there is no damage to the vehicle. These traumatic events can cause damage to the connective tissues that hold the neck and the head within proper boundaries, adversely effecting nerves, blood vessels, lymphatic drainage and the muscles of the head, neck, upper back and jaw. The muscles can remain in a stressed position, which can become the CAUSE of many of the symptoms that originate from this area. Symptoms can be diverse—- with Migraines, Vertigo, TMJ disorders and Face and Neck Pain being just the tip of the iceberg…
What is a very common finding in the cervical spine, following head and neck trauma? The “Lateral” view seen above on the left was taken before the specific upper cervical correction was performed, but shortly after a minor motor vehicle accident—this is the common finding! This otherwise healthy, fit patient had severe spasm of the neck muscles; resulting in a very painful condition we call Spasmodic Torticollis. This X-ray was taken four weeks following a “very minor” car accident wherein the patient slid side-ways into a curb. The damage to the car was minimal. Yet, the patient cannot even raise her head to the normal upright position because the spasms are so intense. The X-ray on the right shows a return of the normal curve. The GOOD NEWS is: These structures can very often be appropriately realigned and when they are, the body will began repairing and healing the injured areas.
The X-ray on the right is the corrected spinal curve, having returned to true normal lordosis following only 5 NUCCA treatments! There were no other modalities performed on this patient. I’ve seen hundreds, if not thousands of cervical curves restored with NUCCA and Atlas Orthogonal (AO). What’s hard for me to fathom, is that Emergency Departments around the country are missing the harm and potential problems that can arise from a reversed or straight neck. The stressed position of the neck as seen on the left is a common finding, and it is often trivialized or dismissed as “normal”. I can see this casual dismissal in some ways. for instance, this important finding is diminished as emergency room staff focus more on “life-threatening” immediate risk problems, and less on conditions and “findings” which might develop into long-term chronic health conditions—it’s simply not their job. Muscle relaxants may be prescribed, but my practical experience in dealing with thousands of patients “after-the-fact” is: taking relaxants will not restore the cervical curve. Further, if left uncorrected, this reversed curve can contribute to the many symptoms and syndromes that are linked to head and neck misalignments, like:
- Headaches of all varieties
- Jaw Joint Dysfunction and Pain, Teeth Pain, Vertigo, Double-Vision
- Neck and Back Pain with chronic Muscle Spasms and Restricted Movement
- Bulging Discs, and more rapidly Advancing Arthritis
- Problems with Clear Thinking or the Ability to Focus
- Heart and Blood Pressure problems
- Poor Posture
- Even Low Back, Hip and Knee Pain
- Depression and Anxiety…. and a whole lot of frustration as “the injured” is bumped around from doctor to doctor with our any real relief..
The most vulnerable area of the spine is where the head rests on the neck. The top bone (called the Atlas) is a small 2-ounce ring-shaped bone with 2 small divots on either side of the spinal cord called facets—these small joints support the full weight of the skull. The adult skull often weighs more than 13 pounds! Imagine—a bowling ball mass being supported by two golf tees! But don’t be fooled—even with what appears to be a “fragile design flaw” in our anatomy, it is quite hardy—except under certain traumatic conditions; then, it can become quite vulnerable to injuries. When this area is fundamentally disturbed through trauma, the head—–and the atlas upon which it rests, lose their normal healthy alignment with one another; the result is a distortion of the spine, the spinal cord and it’s supportive tissues. There is also the possibility of a disturbance of blood flow to and from the brain.
This head and atlas malposition then causes the supporting spinal muscles to contract irregularly in compensation, and will cause the entire spine to distort out-of-balance, thereby effecting the entire body. This upper cervical distortion will almost always result in a high or low hip, a “shortened leg” syndrome ( http://www.myshortleg.com/ ), and usually a high or low shoulder. Often the head will tilt slightly to one side or the other, and the abnormal contraction of the neck muscles will force the normal lordotic curve into a reversed or straightened position—this is COMMON, but not NORMAL. Specific upper cervical X-rays will reveal the misalignment in a multidimensional fashion.
The X-ray views taken following trauma in the Emergency Room, or a doctor’s office will perhaps reveal the reversed curve, but provide little information on what’s causing it or how to fix it.
In my 15 years of practice, I have seen many forms of “therapy” designed to “restore” the normal cervical curve. Some of them you would think were designed more as torture techniques borrowed from a mad scientist laboratory than sound medical restorative therapies. One of the most ludicrous is a technique that situates the back of the neck on a “fulcrum”, while heavy weights are suspended from the forehead using gravity to literally force the head into extension! Well, I can say with certainty: there IS a better way to restore a normal, lordotic neck curve. That way is to get right down to the cause and correct it.
CASE IN POINT:
The X-rays below were taken over a 16-month period. There were only 5 Atlas corrections made over that time period. The X-rays are of a 19-year-old female with a history of gradual onset of neck pain, which became suddenly severe 4 weeks following her sliding side-ways into a curb while traveling as a passenger in a moving vehicle. She estimated her speed to be under 10mph. The front wheel of the car was only “slightly damaged”, and she was quite sure that such a “small bump” could not have caused her severe neck spasms.


Pre-Correction 1st Post-Correction


At 4 Months At 12 Months
Notice in the first view how her head pitches downward due to cervical muscle spasms. The patient could not lift her head any higher than this due to muscle spasms. This is what Spasmodic Torticollis looks like from the side view on an X-ray.
The first “Post” view was taken immediately following the first upper cervical procedure, and you can actually see how the muscle spasms have diminished, allowing the head and neck to begin returning to a normal position. Four months later the head is making progress with only one intervening Orthogonal Atlas adjustment having been performed. Three more Atlas “Corrections” were given over the next 12 months. In the last view, the normal curve has been restored without using contraptions or force.
Gone is the neck pain, the migraines and jaw pain. Happy is the patient!
We may not have turned back the hands of time, but for this young lady who is now 23, we have effectively taken her out of the fast-lane towards spinal degeneration, and essentially saved her from many years of painful struggle.
If you, or someone you know suffers, perhaps that suffering is needless. Don’t wait—we’re here to help.
Authors Note: In the X-rays taken above, a duplication of the patient’s “hard palate angle” seen in the first Post Correction was used as a base line. The author is aware that, though not “on level” as is the measuring convention, it was important to maintain the initial sloped palate angle in order to accurately compare subsequent X-rays as raising up the angle would induce an artifactual increase in curve.
Bio: Doctor Christopher Chapman is a graduate of Palmer College of Chiropractic and is a Board Certified Chiropractic Physician. He practices exclusively the Atlas Orthogonal (AO) and NUCCA procedures in Provo, Utah using certified aligned X-ray equipment. He has published articles on the etiology of Atlas Subluxation, lectures nationally to a multidisciplinary audience of dentists, chiropractors and is pioneering orthogonal based spinal procedures in association with leading researchers in the field of Epigenetics. He is the Clinic Director for the Chapman Clinic for Spinal and Craniofacial Epigenetics and currently instructs and mentors Associate Doctors interested in perfecting the clinical application of the Atlas Orthogonal procedure. NUCCA Spinal Centers is an authorized internship facility associated with Brigham Young University. Interns from this program have gone on to study chiropractic, hoping to eventually specialize in the Orthogonal based upper cervical techniques. Telephone consultations are available by calling 801.655.1801.
From Medscape Medical News
Migraine With Aura Linked to Increased Mortality From Stroke and Heart Disease
Fran Lowry
August 26, 2010 — Migraine, particularly migraine with aura, is associated with an increased risk for death from cardiovascular disease and hemorrhagic stroke, according to the findings of 2 large prospective cohort studies.
But, the researchers emphasize, the individual risk for those with migraine is low. The reports, which add more weight to previous data suggesting this link, were published online August 25 in the British Medical Journal.
Reykjavik Study
In the first study, Larus S. Gudmundsson, a doctoral student from the University of Iceland in Reykjavik, and colleagues assessed the impact of midlife migraine episodes in 18,725 men and women born between 1907 and 1935.
The study cohort was part of the Reykjavik Study, which was started in 1967 by the Icelandic Heart Association to prospectively study cardiovascular disease in Iceland. Participants were followed up for up to 40 years, until the end of 2007. The median follow-up was 25.9 years. In total, the researchers assessed 470,990 person-years of data and used questionnaires to assess migraine with and without aura.
Overall, there were 10,358 deaths, 4323 from cardiovascular disease and 6035 from other causes.
After adjusting for baseline risk factors, age, and sex, the study found that people with migraine with aura were at increased risk for all-cause mortality and mortality from cardiovascular disease compared with people with no headache. No increased risk was found for people with migraine without aura and people with nonmigraine headache.
A closer look at death from cardiovascular disease revealed that people with migraine with aura were at increased risk for mortality from coronary heart disease and stroke.
Table. Mortality Risk for Migraine With Aura vs No Headache
CI = confidence interval
The study also showed that women with migraine with aura were at increased risk for mortality from noncardiovascular disease (hazard ratio, 1.19; 95% confidence interval, 1.06 – 1.35).
Explaining the clinical significance of the findings, Gudmundsson told Medscape Medical News, “Although our study shows that migraine and in particular migraine with aura is an independent risk factor for all-cause and cardiovascular disease mortality, the risk is low compared to conventional modifiable risk factors, such as smoking, adverse blood lipid profile, and hypertension. Having migraine with aura should be an additional reason for monitoring your modifiable risk factors and keeping them in check, and this applies to both men and women.”
He added that future studies will determine whether reducing migraine or aura frequency with medication or other interventions will lower the risk for cardiovascular disease in these individuals. [emphasis added]
Comments from Dr. Chapman:
More and more studies are showing the potential relationship between various pathologies and disorders. Here we have two major “players” when it comes to human suffering; migraines with aura and an increases in mortality not only from stroke, but due to other “non-cardiovascular related disorders”.
This very long and careful study clearly shows the correlation between Aura Associated Migraines (AAM) and mortality from cardiovascular disease, like stroke—but it also makes a finer more interesting point: The study could draw our thinking into more holistic and connected patterns of clinical reasoning, wherein we as physicians, might begin to make some fundamental observations about the potential common causes of disease.
Understanding this could create a new discussion for treatment. For instance, NUCCA research has shown a clear relationship between hypertension and the Atlas subluxation (see WebMD article: http://www.webmd.com/hypertension-high-blood-pressure/news/20070316/chiropractic-cuts-blood-pressure ). It also shows a correlation between Atlas subluxation and headaches of all varieties, including migraines with and without aura. (See Journal of Man. Ther. 1999; 7(1):33-39, Man. Physiol Ther, 1980; 3(3):137, Cephalgia 1987; 7(2):147-160) The Reykjavik Study suggests that both migraines and hypertension may be a different tangent of expression by the body for potentially the same underlying problem or condition. “Chronic Anything” indicates some underlying imbalance.
So, if we follow this clinical reasoning, then potentially correcting the underlying problem which is CAUSING both migraines and hypertension could lead to a reduction in mortality rates. (Wisely, the author left the notion on the table that “interventions”, (including drugs of course) in the conditions may reduce risks, thereby reducing mortality rates) In plain English—you just may live longer and happier when you are in proper spinal alignment–without drugs.
Migraine With Aura Linked to Increased Mortality From Stroke and Heart Disease
Fran Lowry
August 26, 2010 — Migraine, particularly migraine with aura, is associated with an increased risk for death from cardiovascular disease and hemorrhagic stroke, according to the findings of 2 large prospective cohort studies.
But, the researchers emphasize, the individual risk for those with migraine is low. The reports, which add more weight to previous data suggesting this link, were published online August 25 in the British Medical Journal.
Reykjavik Study
In the first study, Larus S. Gudmundsson, a doctoral student from the University of Iceland in Reykjavik, and colleagues assessed the impact of midlife migraine episodes in 18,725 men and women born between 1907 and 1935.
The study cohort was part of the Reykjavik Study, which was started in 1967 by the Icelandic Heart Association to prospectively study cardiovascular disease in Iceland. Participants were followed up for up to 40 years, until the end of 2007. The median follow-up was 25.9 years. In total, the researchers assessed 470,990 person-years of data and used questionnaires to assess migraine with and without aura.
Overall, there were 10,358 deaths, 4323 from cardiovascular disease and 6035 from other causes.
After adjusting for baseline risk factors, age, and sex, the study found that people with migraine with aura were at increased risk for all-cause mortality and mortality from cardiovascular disease compared with people with no headache. No increased risk was found for people with migraine without aura and people with nonmigraine headache.
A closer look at death from cardiovascular disease revealed that people with migraine with aura were at increased risk for mortality from coronary heart disease and stroke.
Table. Mortality Risk for Migraine With Aura vs No Headache
| Endpoint | Adjusted Hazard Ratio (95% CI) |
| All-cause mortality | 1.21 (1.12 – 1.30) |
| Cardiovascular disease mortality | 1.27 (1.13 – 1.43) |
| Coronary heart disease mortality | 1.28 (1.11 – 1.49) |
| Stroke mortality | 1.40 (1.10 – 1.78) |
The study also showed that women with migraine with aura were at increased risk for mortality from noncardiovascular disease (hazard ratio, 1.19; 95% confidence interval, 1.06 – 1.35).
Explaining the clinical significance of the findings, Gudmundsson told Medscape Medical News, “Although our study shows that migraine and in particular migraine with aura is an independent risk factor for all-cause and cardiovascular disease mortality, the risk is low compared to conventional modifiable risk factors, such as smoking, adverse blood lipid profile, and hypertension. Having migraine with aura should be an additional reason for monitoring your modifiable risk factors and keeping them in check, and this applies to both men and women.”
He added that future studies will determine whether reducing migraine or aura frequency with medication or other interventions will lower the risk for cardiovascular disease in these individuals. [emphasis added]
Comments from Dr. Chapman:
More and more studies are showing the potential relationship between various pathologies and disorders. Here we have two major “players” when it comes to human suffering; migraines with aura and an increases in mortality not only from stroke, but due to other “non-cardiovascular related disorders”.
This very long and careful study clearly shows the correlation between Aura Associated Migraines (AAM) and mortality from cardiovascular disease, like stroke—but it also makes a finer more interesting point: The study could draw our thinking into more holistic and connected patterns of clinical reasoning, wherein we as physicians, might begin to make some fundamental observations about the potential common causes of disease.
Understanding this could create a new discussion for treatment. For instance, NUCCA research has shown a clear relationship between hypertension and the Atlas subluxation (see WebMD article: http://www.webmd.com/hypertension-high-blood-pressure/news/20070316/chiropractic-cuts-blood-pressure ). It also shows a correlation between Atlas subluxation and headaches of all varieties, including migraines with and without aura. (See Journal of Man. Ther. 1999; 7(1):33-39, Man. Physiol Ther, 1980; 3(3):137, Cephalgia 1987; 7(2):147-160) The Reykjavik Study suggests that both migraines and hypertension may be a different tangent of expression by the body for potentially the same underlying problem or condition. “Chronic Anything” indicates some underlying imbalance.
So, if we follow this clinical reasoning, then potentially correcting the underlying problem which is CAUSING both migraines and hypertension could lead to a reduction in mortality rates. (Wisely, the author left the notion on the table that “interventions”, (including drugs of course) in the conditions may reduce risks, thereby reducing mortality rates) In plain English—you just may live longer and happier when you are in proper spinal alignment–without drugs.
Hitting a Nerve – TMD
We need to keep this thought in mind: “The optimal treatment of the jaw joints and occlusion (bite related issues) should be performed in the context of a balanced upper cervical spine and head. The NUCCA procedure restores this essential balance. It is clear from my clinical experience that TMD disorders, even advanced cases respond well with NUCCA treatment.”
Malpositions of the head and neck are often associated with a common jaw disorder called Temporomandibular Joint (TMJ) Dysfunction, or TMD. TMD is also known as TMJ Syndrome. The jaw joint is a hinge joint which is literally suspended and anchored in its normal position by the muscles of the head, neck and shoulder.

The “Jaw Joint” or TMJ
TMD Syndrome occurs when the normal functional position of the jaw joints shift into an irregular position and a grinding use-pattern develops. This abnormal use-pattern and position can cause the sufferer of the syndrome a significant amount of pain and inflammation, making chewing, sleeping and even speaking difficult. The pain symptoms are quite diverse. Jaw disorders can refer pain to the head, neck and upper back. Pain can also be felt in the face and in the teeth. Conventional dental treatments can be quite expensive and time intensive, and can range in price from $5,000 to $50,000 upwards, and include surgeries, electrical stimulation and medication for pain.
At NUCCA Spinal Centers, under the precision care standard of the NUCCA procedure, TMD sufferers often find significant and lasting relief upon the first correction.
My clinical protocols have resolved TMD and its associated syndromes for hundreds of patients over the last 12 years. TMJ disorders should be assessed in the context of the entire head and neck region, and therefore may be viewed clinically as “a side-effect of a structural dysfunction stemming from the head and neck mislalignment“. So, TMD can be addressed effectively by addressing an underlying imbalance.
Essentially, what I have found is: TMD treatments utilizing NUCCA protocols as a core corrective procedure have been highly successful. Another thing I have observed is: when the patients head and neck are restored to a normal aligned position through the NUCCA procedure, this restoration significantly enhances the patient’s TMD dental protocols and treatment, and, in a high number of cases, can entirely resolve the syndrome within several weeks of the NUCCA procedure.
If you are dealing with a TMJ issue or jaw pain presently, and whether you are working with a dentist or not, I advise you to come in for an examination/consultation, and, if it is appropriate, I will be happy to speak to your dental specialist about the NUCCA procedure and discuss how it could positively impact your therapy. I work closely with several dental specialists in Utah and Salt Lake Counties when combined interventions and treatment are needed.
Telephone consultations are available.
Doctor Christopher Chapman is a graduate of Palmer College of Chiropractic, and is a Board Certified Chiropractic Physician. He practices exclusively the NUCCA procedure in Provo, Utah using certified aligned X-ray equipment. He is the Clinic Director for Balance Point Clinics, Inc.—dba—NUCCA Spinal Centers and currently instructs and mentors Associate doctors interested in perfecting the clinical application of the NUCCA procedure. NUCCA Spinal Centers is a registered internship facility and correlates field study for interested and qualified health professionals in association with Brigham Young University. Candidates for this Internship program have gone on to study chiropractic, hoping to eventually specialize in the NUCCA technique. Currently Dr. Chapman is writing a book describing the essential role posture and structural balance plays in human health.
We need to keep this thought in mind: “The optimal treatment of the jaw joints and occlusion (bite related issues) should be performed in the context of a balanced upper cervical spine and head. The NUCCA procedure restores this essential balance. It is clear from my clinical experience that TMD disorders, even advanced cases respond well with NUCCA treatment.”
Malpositions of the head and neck are often associated with a common jaw disorder called Temporomandibular Joint (TMJ) Dysfunction, or TMD. TMD is also known as TMJ Syndrome. The jaw joint is a hinge joint which is literally suspended and anchored in its normal position by the muscles of the head, neck and shoulder.

The “Jaw Joint” or TMJ
TMD Syndrome occurs when the normal functional position of the jaw joints shift into an irregular position and a grinding use-pattern develops. This abnormal use-pattern and position can cause the sufferer of the syndrome a significant amount of pain and inflammation, making chewing, sleeping and even speaking difficult. The pain symptoms are quite diverse. Jaw disorders can refer pain to the head, neck and upper back. Pain can also be felt in the face and in the teeth. Conventional dental treatments can be quite expensive and time intensive, and can range in price from $5,000 to $50,000 upwards, and include surgeries, electrical stimulation and medication for pain.
At NUCCA Spinal Centers, under the precision care standard of the NUCCA procedure, TMD sufferers often find significant and lasting relief upon the first correction.
My clinical protocols have resolved TMD and its associated syndromes for hundreds of patients over the last 12 years. TMJ disorders should be assessed in the context of the entire head and neck region, and therefore may be viewed clinically as “a side-effect of a structural dysfunction stemming from the head and neck mislalignment“. So, TMD can be addressed effectively by addressing an underlying imbalance.
Essentially, what I have found is: TMD treatments utilizing NUCCA protocols as a core corrective procedure have been highly successful. Another thing I have observed is: when the patients head and neck are restored to a normal aligned position through the NUCCA procedure, this restoration significantly enhances the patient’s TMD dental protocols and treatment, and, in a high number of cases, can entirely resolve the syndrome within several weeks of the NUCCA procedure.
If you are dealing with a TMJ issue or jaw pain presently, and whether you are working with a dentist or not, I advise you to come in for an examination/consultation, and, if it is appropriate, I will be happy to speak to your dental specialist about the NUCCA procedure and discuss how it could positively impact your therapy. I work closely with several dental specialists in Utah and Salt Lake Counties when combined interventions and treatment are needed.
Telephone consultations are available.
Doctor Christopher Chapman is a graduate of Palmer College of Chiropractic, and is a Board Certified Chiropractic Physician. He practices exclusively the NUCCA procedure in Provo, Utah using certified aligned X-ray equipment. He is the Clinic Director for Balance Point Clinics, Inc.—dba—NUCCA Spinal Centers and currently instructs and mentors Associate doctors interested in perfecting the clinical application of the NUCCA procedure. NUCCA Spinal Centers is a registered internship facility and correlates field study for interested and qualified health professionals in association with Brigham Young University. Candidates for this Internship program have gone on to study chiropractic, hoping to eventually specialize in the NUCCA technique. Currently Dr. Chapman is writing a book describing the essential role posture and structural balance plays in human health.
Healing the body may actually start by healing the mind.
Just this morning I received this message on my Facebook from a patient whom I had seen in the clinic on Friday:
“I seem to have taken a turn for the worse. My head has a splitting head ache. I have pain between my shoulder blades. I have not thrown up yet. I have no organ pain. So I do not think iyt has anything to do with the pancreas, liver, or gall bladder. The diarrhea has not let up. I get waves of stomach cramps after sipping water or eating. I have been having muscle cramps. Once it was my left hand thumb cramped to the hand would not move, it was painful and then it opened. Once my left abdomen the muscle cramped until I put my hand on it and relaxed it. Sometimes even my heart hurts. Sounds like dehydration and mineral depletion. My body does not respond to PB8 so I cannot [imagine] it metabolizing minerals. I simply do not know what to do. It is the holiday weekend and I do not know what to do. Any suggestions[?]”
That message and the telephone conversation we had this morning after I called her provoked the explanation below.
I have often witnessed that symptomatically some of my patients seem to get worse before they get better—and truthfully, this has caused me some consternation in the past. But, I have come to realize that the body has ways of expressing healing that are not all pixie dust and warm fuzzies. Some of the cleansing/healing processes can be a little itchy-scratchy—and painful. Some can be downright terrifying. Understanding what the body is doing and decoding the symptoms correctly is a key step in healing the mind, hence, keeping the body on track.
The human mind deals in code, and language is the code of the mind. The body also deals in code. The sensory parts of the body transmit coded messages to the brain, and those coded messages are detected by the brain through our nervous system. It is the mind—not merely the brain—that must decipher these codes and make judgments about them. The mind asks the question: Am I dying? Or, am I healing? In some cases, it can feel grossly similar…. This is where the code of language can help. The mind simply needs to be reassured that the body is healing rather than dying. (Let me say that I am not suggesting that in acute medical emergencies, like stroke or myocardial infarction, wherein a patient is in dire need of interventive care that simply tricking the brain into believing that it is healing rather than dying is the remedial path. Clearly, I am not saying that…) But in situations where healing has begun and the patient is unsure—THIS is where a caring helper and facilitator (like a doctor) comes into play. This, I feel, is the essence of being a doctor. Being a doctor is sort of like being a “seeing eye dog”—sans the flees… During the first few steps towards healing, our patients rely more heavily upon us until they gain their footing on the path. They need not only remedial procedures, but they need to be taught what is happening inside their own bodies and shown what it really means. They need a discerning eye to help them to interpret the body codes.
I am going to give an example. Say you have a person present with a constellation of symptoms ranging from.
There are several layers of issues and complexities that you are dealing with as a physician—from mind to toe. Clearly, there are likely some chronic musculoskeletal issues going on with the older injuries. There are chronic issues of emotional stress on the system and the wear and tear associated with that silent killer. There is the issue of recent, compounded upon the chronic gastric distress. There is some acute distress and inflammation from the recent trauma. So there is understandably the emotional lability that comes from having to live in the context of this suffering from day to day without relief or answers.
What to do, what to do….? The question we face on every patient———every encounter.
In my first blog, my “welcome to the mending path”, I mentioned that the body has numerous mechanisms for dealing the stimuli which cause a state of dis-ease in the body. Stimuli can be an internal encounter with some “thing” like a toxin, or, it can be an external encounter like our encounter with a belief. The effects of either can and often will manifest in the body. The body has many defense mechanisms. One of these is compartmentalization. This is where the body may “wall-off” a disaster area. This can occur cellularly or systemically…. it can even occur psychologically. If the burden on the system is greater than the ability of the system to buffer, or dispose of, or effectively mitigate the destabilizing effects of a noxious stimuli, they will simply build-up or accumulate until naturally dispelled through some process—or, sadly until it kills us. (Clearly not an option for my patients) As the body deals with the load of harmful stimuli it must have a way to express or spill off the bi-products. Since the body has an on-board program to maintain a state of homeostasis or balance, it would stand to reason that it would use its various systems to facilitate this. And in fact, it does quite a nice job of this most of the time unless is becomes overburdened. Overburdening means that the mitigating/balancing mechanisms innate to the body cannot keep pace with the stresses placed upon them. This results in a state of dis-ease. We could use the metaphor of the body being like a bathtub with a drain. The bathtub has a capacity to hold a certain quantity of water, but likes to keep the level relatively unchanged and at a certain balanced midpoint. That point is like homeostasis, meaning a point of equilibrium or balance of the systems. The bathtub has a source for water (input) and it has a means of draining the water (output). If the output can keep pace with the input and keep the water level on the balance point mark, then all is well in the system. But, IF the input exceeds the drain output, then the water starts to build to a point where it must dissipate by spilling over the tub edge. When the water starts rising beyond the balance point, it may start to get our attention by alerting us to the subtle disturbances reverberating in the system—but maybe not…. In our body, these disturbances come in form of subtle symptoms and signs. This is the perfect time to call the plumber right? Ideally, yes. But usually the plumber is not called until after the first flood, or maybe the second one… just human nature. Part of the reason for that is we don’t know where to turn for understanding.
So once the plumber is called, they can get to work on solving the problem.
In the case of this patient, I was the plumber she finally called. (Bear in mind, I was not the first plumber she called on these issues) So, from the perspective of a NUCCA doctor, I made certain assessments and determine that a particular intervention was needful.
I took specific X-rays of the head and neck determined that the patients Atlas was severely subluxated—in other words, “not in the right place”, and that was causing the following:
It is spring time. Many of us are cleaning out attics, garages, cars, etc. We may even be clearing out harmful relationships. When the body embarks upon a mending path, it can be just as pleasant as cleaning out a septic tank. So, when in the midst of the muck of the mire—know that you are coming out of it rather than settling into it. That proper interpretation of the unpleasant codes produced by the body can make all the difference to the mind.
Try to enjoy the journey…
Just this morning I received this message on my Facebook from a patient whom I had seen in the clinic on Friday:
“I seem to have taken a turn for the worse. My head has a splitting head ache. I have pain between my shoulder blades. I have not thrown up yet. I have no organ pain. So I do not think iyt has anything to do with the pancreas, liver, or gall bladder. The diarrhea has not let up. I get waves of stomach cramps after sipping water or eating. I have been having muscle cramps. Once it was my left hand thumb cramped to the hand would not move, it was painful and then it opened. Once my left abdomen the muscle cramped until I put my hand on it and relaxed it. Sometimes even my heart hurts. Sounds like dehydration and mineral depletion. My body does not respond to PB8 so I cannot [imagine] it metabolizing minerals. I simply do not know what to do. It is the holiday weekend and I do not know what to do. Any suggestions[?]”
That message and the telephone conversation we had this morning after I called her provoked the explanation below.
I have often witnessed that symptomatically some of my patients seem to get worse before they get better—and truthfully, this has caused me some consternation in the past. But, I have come to realize that the body has ways of expressing healing that are not all pixie dust and warm fuzzies. Some of the cleansing/healing processes can be a little itchy-scratchy—and painful. Some can be downright terrifying. Understanding what the body is doing and decoding the symptoms correctly is a key step in healing the mind, hence, keeping the body on track.
The human mind deals in code, and language is the code of the mind. The body also deals in code. The sensory parts of the body transmit coded messages to the brain, and those coded messages are detected by the brain through our nervous system. It is the mind—not merely the brain—that must decipher these codes and make judgments about them. The mind asks the question: Am I dying? Or, am I healing? In some cases, it can feel grossly similar…. This is where the code of language can help. The mind simply needs to be reassured that the body is healing rather than dying. (Let me say that I am not suggesting that in acute medical emergencies, like stroke or myocardial infarction, wherein a patient is in dire need of interventive care that simply tricking the brain into believing that it is healing rather than dying is the remedial path. Clearly, I am not saying that…) But in situations where healing has begun and the patient is unsure—THIS is where a caring helper and facilitator (like a doctor) comes into play. This, I feel, is the essence of being a doctor. Being a doctor is sort of like being a “seeing eye dog”—sans the flees… During the first few steps towards healing, our patients rely more heavily upon us until they gain their footing on the path. They need not only remedial procedures, but they need to be taught what is happening inside their own bodies and shown what it really means. They need a discerning eye to help them to interpret the body codes.
I am going to give an example. Say you have a person present with a constellation of symptoms ranging from.
- Gastrointestinal distress such as stomach pain, vomiting and diarrhea.
- Musculoskeletal pain in all four limbs and in the back, neck and head.
- Abnormal sensations in the hands and feet.
- Postural distortions in sitting and standing positions.
- Sensory disturbances like vertigo and sensitivity to light.
- Anxiety over finances and inability to keep commitments due to health challenges.
- Anxiety over the meaning of the symptoms themselves: “Is it my heart? Am I dying? What is really wrong? What am I going to do? Who can help me? Essential queries that produce fear and more anxiety rather than peace and reassurance.
There are several layers of issues and complexities that you are dealing with as a physician—from mind to toe. Clearly, there are likely some chronic musculoskeletal issues going on with the older injuries. There are chronic issues of emotional stress on the system and the wear and tear associated with that silent killer. There is the issue of recent, compounded upon the chronic gastric distress. There is some acute distress and inflammation from the recent trauma. So there is understandably the emotional lability that comes from having to live in the context of this suffering from day to day without relief or answers.
What to do, what to do….? The question we face on every patient———every encounter.
In my first blog, my “welcome to the mending path”, I mentioned that the body has numerous mechanisms for dealing the stimuli which cause a state of dis-ease in the body. Stimuli can be an internal encounter with some “thing” like a toxin, or, it can be an external encounter like our encounter with a belief. The effects of either can and often will manifest in the body. The body has many defense mechanisms. One of these is compartmentalization. This is where the body may “wall-off” a disaster area. This can occur cellularly or systemically…. it can even occur psychologically. If the burden on the system is greater than the ability of the system to buffer, or dispose of, or effectively mitigate the destabilizing effects of a noxious stimuli, they will simply build-up or accumulate until naturally dispelled through some process—or, sadly until it kills us. (Clearly not an option for my patients) As the body deals with the load of harmful stimuli it must have a way to express or spill off the bi-products. Since the body has an on-board program to maintain a state of homeostasis or balance, it would stand to reason that it would use its various systems to facilitate this. And in fact, it does quite a nice job of this most of the time unless is becomes overburdened. Overburdening means that the mitigating/balancing mechanisms innate to the body cannot keep pace with the stresses placed upon them. This results in a state of dis-ease. We could use the metaphor of the body being like a bathtub with a drain. The bathtub has a capacity to hold a certain quantity of water, but likes to keep the level relatively unchanged and at a certain balanced midpoint. That point is like homeostasis, meaning a point of equilibrium or balance of the systems. The bathtub has a source for water (input) and it has a means of draining the water (output). If the output can keep pace with the input and keep the water level on the balance point mark, then all is well in the system. But, IF the input exceeds the drain output, then the water starts to build to a point where it must dissipate by spilling over the tub edge. When the water starts rising beyond the balance point, it may start to get our attention by alerting us to the subtle disturbances reverberating in the system—but maybe not…. In our body, these disturbances come in form of subtle symptoms and signs. This is the perfect time to call the plumber right? Ideally, yes. But usually the plumber is not called until after the first flood, or maybe the second one… just human nature. Part of the reason for that is we don’t know where to turn for understanding.
So once the plumber is called, they can get to work on solving the problem.
In the case of this patient, I was the plumber she finally called. (Bear in mind, I was not the first plumber she called on these issues) So, from the perspective of a NUCCA doctor, I made certain assessments and determine that a particular intervention was needful.
I took specific X-rays of the head and neck determined that the patients Atlas was severely subluxated—in other words, “not in the right place”, and that was causing the following:
- a slight distortion of the spinal cord,
- interference in the vascular supply and drainage to and from the brain,
- and broad primary muscular imbalances of the entire spine and pelvis.
It is spring time. Many of us are cleaning out attics, garages, cars, etc. We may even be clearing out harmful relationships. When the body embarks upon a mending path, it can be just as pleasant as cleaning out a septic tank. So, when in the midst of the muck of the mire—know that you are coming out of it rather than settling into it. That proper interpretation of the unpleasant codes produced by the body can make all the difference to the mind.
Try to enjoy the journey…
Older posts
No comments:
Post a Comment