Cervical Myelopathy
Topic updated on 01/28/16 5:06pm
| Introduction |
 A clinical syndrome caused by compression on the spinal cord that is characterized by A clinical syndrome caused by compression on the spinal cord that is characterized by
- clumsiness in hands
- gait imbalance
- Pathophysiology
- etiology
- degenerative cervical spondylosis (CSM)

- most common cause of cervical myelopathy
- compression usually caused by anterior degenerative changes (osteophytes, discosteophyte complex)
- degenerative spondylolisthesis and hypertrophy of ligamentum flavum may contribute
- congenital stenosis
- symptoms usually begin when congenital narrowing combined with spondylotic degenerative changes in older patients
- OPLL
- tumor
- epidural abscess
- trauma
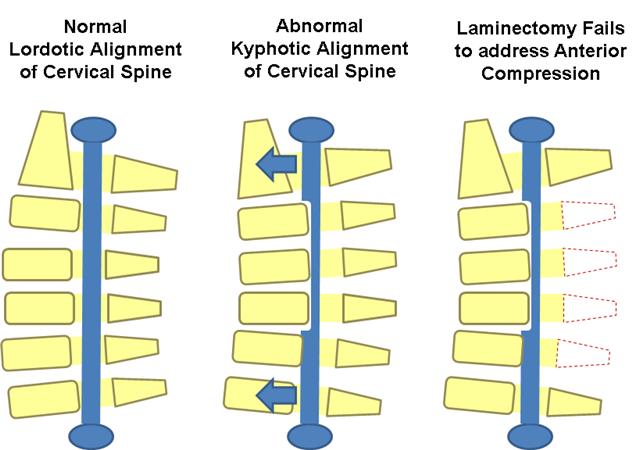
- cervical kyphosis
- neurologic injury
- mechanism of injury can be
- direct cord compression
- ischemic injury secondary to compression of anterior spinal artery
- Associated conditions
- lumbar spinal stenosis

- tandem stenosis occurs in lumbar and cervical spine in ~20% of patients
- Prognosis
- natural history
- tends to be slowly progressive and rarely improves with nonoperative modalities
- progression characterized by steplike deterioration with periods of stable symptoms
- prognosis
- early recognition and treatment prior to spinal cord damage is critical for good clinical outcomes
|
| Classification of Myelopathy |
| |
| Nurick Classification |
| Grade 0 | Root symptoms only or normal |
| Grade 1 | Signs of cord compression; normal gait |
| Grade 2 | Gait difficulties but fully employed |
| Grade 3 | Gait difficulties prevent employment, walks unassisted |
| Grade 4 | Unable to walk without assistance |
| Grade 5 | Wheelchair or bedbound |
Based on gait and ambulatory function  |
|
| |
| Ranawat Classification |
| Class I | Pain, no neurologic deficit |
| Class II | Subjective weakness, hyperreflexia, dyssthesias |
| Class IIIA | Objective weakness, long tract signs, ambulatory |
| Class IIIB | Objective weakness, long tract signs, non-ambulatory |
|
| |
| Japanese Orthopaedic Association Classification |
- A point scoring system (17 total) based on function in the following categories

- upper extremity motor function
- lower extremity motor function
- sensory function
- bladder function
|
|
| |
| Presentation of Myelopathy |
- Symptoms
- neck pain and stiffness
- axial neck pain (often times absent)
- occipital headache common
- extremity paresthesias
- diffuse nondermatomal numbness and tingling
- weakness and clumsiness
- weakness and decreased manual dexterity (dropping object, difficulty manipulating fine objects)
- gait instability
- patient feels "unstable" on feet
- weakness walking up and down stairs
- gait changes are most important clinical predictor
- urinary retention
- rare and only appear late in disease progression
- not very useful in diagnosis due to high prevalence of urinary conditions in this patient population
- Physical exam
- motor
- weakness
- usually difficult to detect on physical exam
- lower extremity weakness is a more concerning finding
- finger escape sign
- when patient holds fingers extended and adducted, the small finger spontaneously abducts due to weakness of intrinsic muscle
- grip and release test
- normally a patient can make a fist and release 20 times in 10 seconds. myelopathic patients may struggle to do this
- sensory
- proprioception dysfunction
- due to dorsal column involvement
- occurs in advanced disease
- associated with a poor prognosis
- decreased pain sensation
- pinprick testing should be done to look for global decrease in sensation or dermatomal changes
- due to involvement of lateral spinothalamic tract
- vibratory changes are usually only found in severe case of long-standing myelopathy
- upper motor neuron signs (spasticity)

- hyperreflexia
- may be absent when there is concomitant peripheral nerve disease (cervical or lumbar nerve root compression, spinal stenosis, diabetes)
- inverted radial reflex
- tapping distal brachioradialis tendon produces ipsilateral finger flexion
- Hoffmann's sign
 
- snapping patients distal phalanx of middle finger leads to spontaneous flexion of other fingers
- sustained clonus
- > three beats defined as sustained clonus
- sustained clonus has poor sensitivity (~13%) but high specificity (~100%) for cervical myelopathy
- Babinski test
- considered positive with extension of great toe
- gait and balance
- toe-to-heel walk
- patient has difficulty performing
- Romberg test
- patient stands with arms held forward and eyes closed
- loss of balance consistent with posterior column dysfunction
- provocative tests
- Lhermitte Sign

- test is positive when extreme cervical flexion leads to electric shock-like sensations that radiate down the spine and into the extremities
|
| Evaluation |
- Radiographs
- recommended views
- cervical AP, lateral, oblique, flexion, and extension views
- general findings
- degenerative changes of uncovertebral and facet joints
- osteophyte formation
- disc space narrowing
- decreased sagittal diameter
- cord compression occurs with canal diameter is < 13mm
- lateral radiograph
- important to look for diameter of spinal canal
- a Pavlov ratio of less than 0.8 suggest a congenitally narrow spinal canal predisposing to stenosis and cord compression
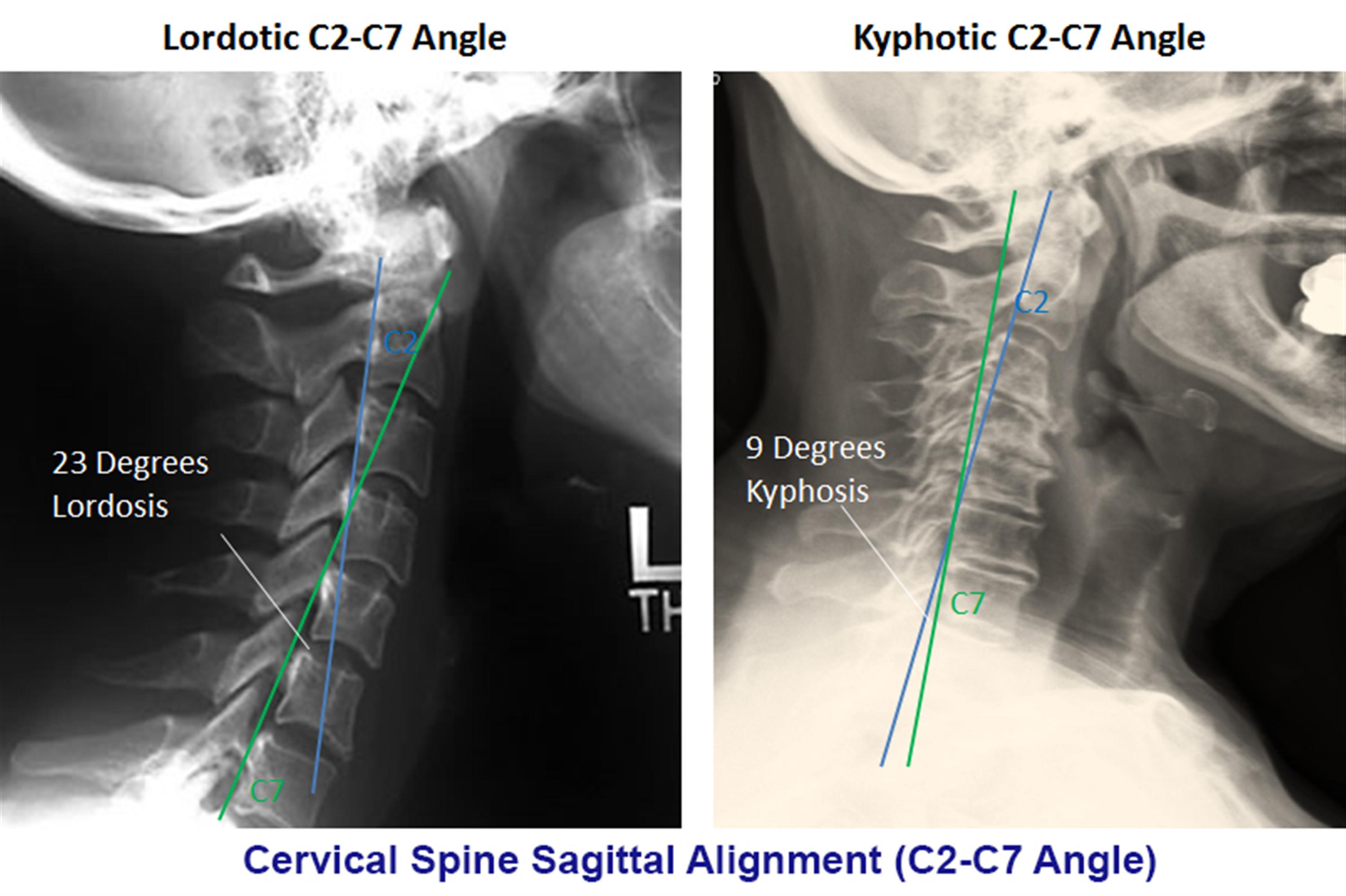
- sagittal alignment
- C2 to C7 alignment

- determined by tangential lines on the posterior edge of the C2 and C7 body on lateral radiographs in neutral position
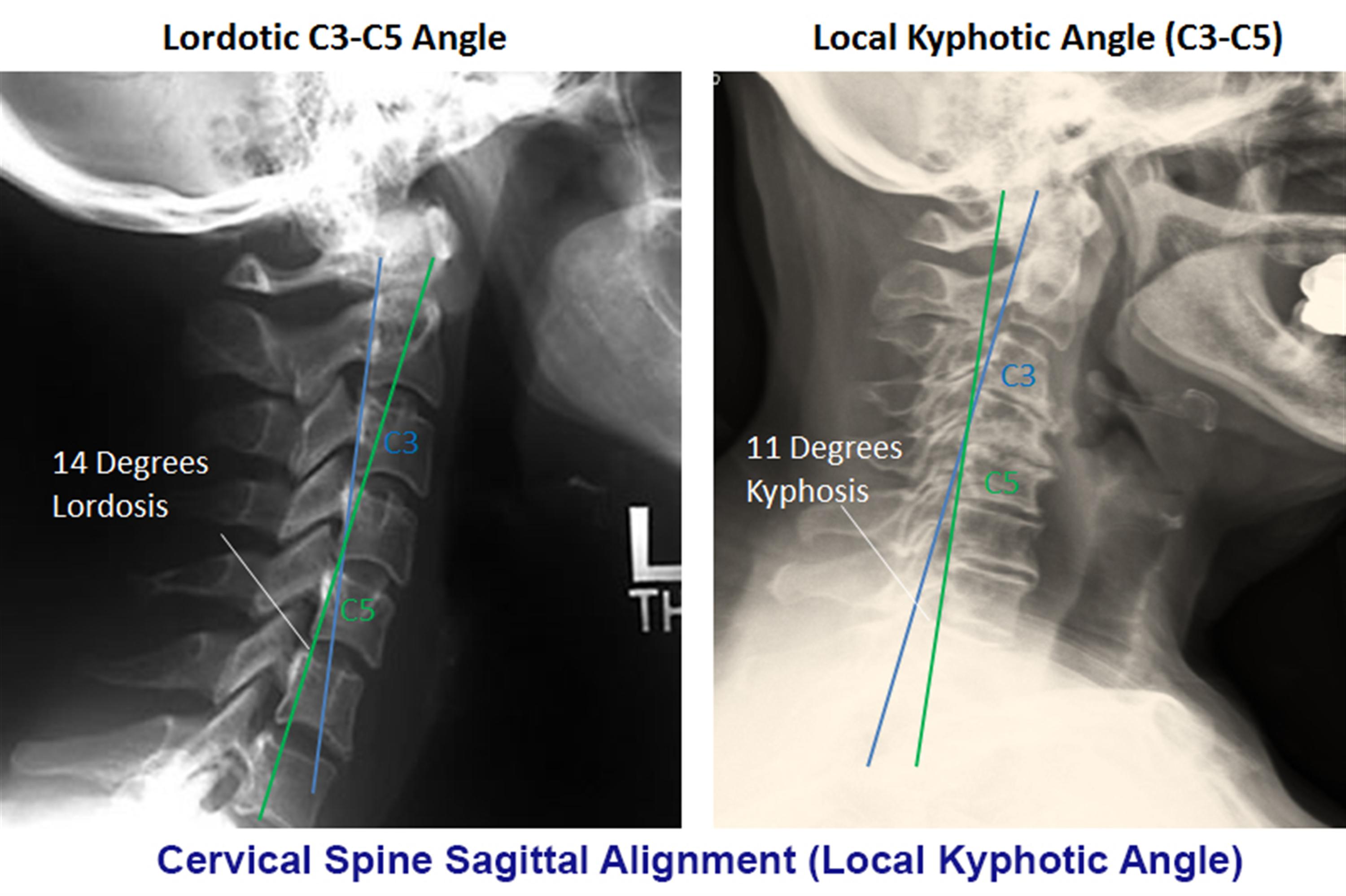
- local kyphosis angle
- the angle between the lines drawn at the posterior margin of most cranial and caudal vertebral bodies forming the maximum local kyphosis
- oblique radiograph
- important to look for foraminal stenosis which often caused by uncovertebral joint arthrosis
- flexion and extension views
- important to look for angular or translational instability
- look for compensatory subluxation above or below the spondylotic/stiff segment
- sensitivity/specificity
- changes often do not correlate with symptoms
- 70% of patients by 70 yrs of age will have degenerative changes seen on plain xrays
- MRI
- indications
- MRI is study of choice to evaluate degree of spinal cord and nerve root compression
- findings
- effacement of CSF indicates functional stenosis
- spinal cord signal changes
- seen as bright signal on T2 images (myelomalacia)

- signal changes on T1-weighted images correlate with a poorer prognosis following surgical decompression
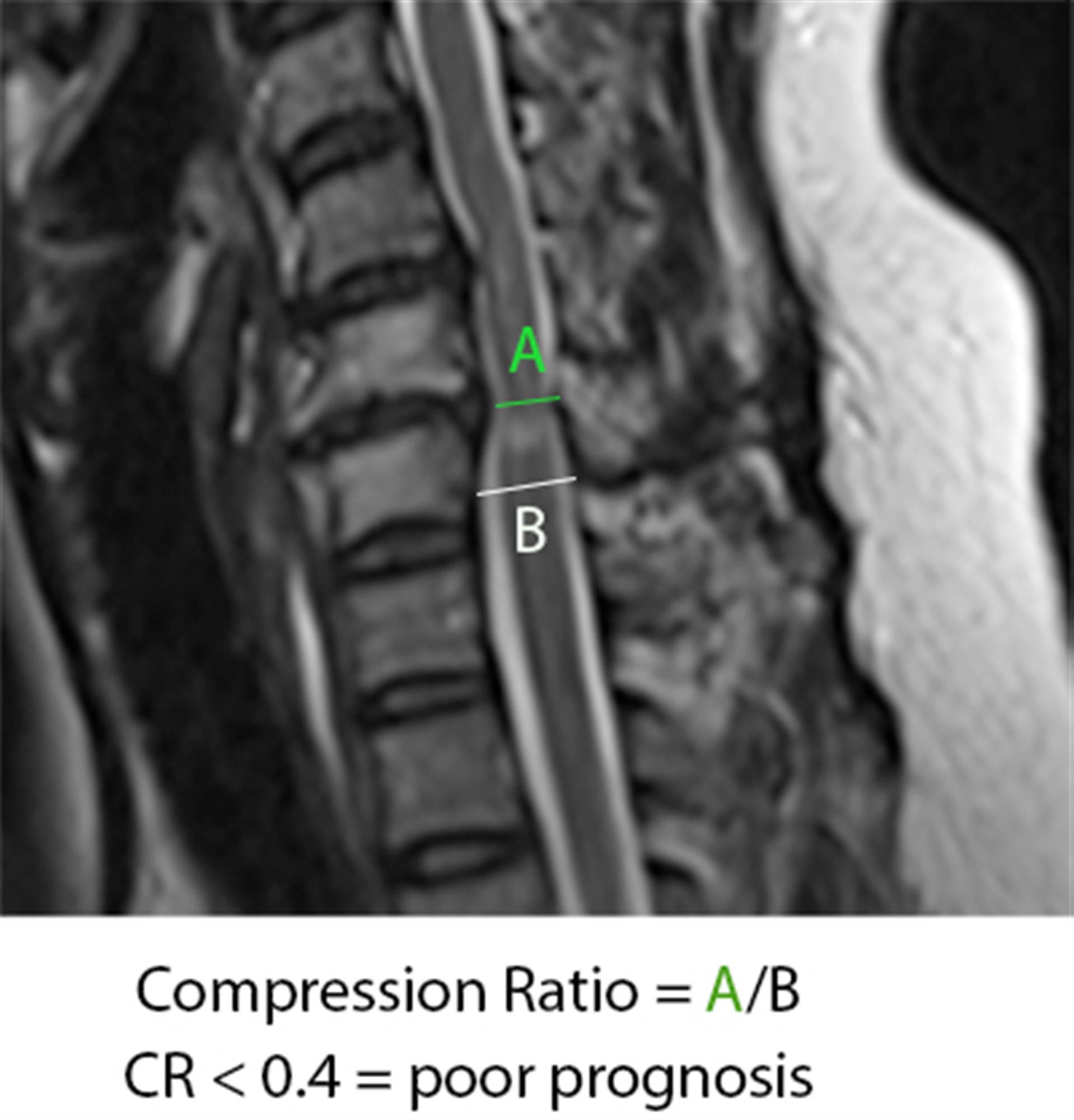
- compression ratio of < 0.4 carries poor prognosis
- CR = smallest AP diameter of cord / largest transverse diameter of cord
- sensitivity/specificity
- has high rate of false positive (28% greater than 40 will have findings of HNP or foraminal stenosis)
- CT without contrast
- can provide complementary information with an MRI, and is more useful to evaluate OPLL and osteophytes
- CT myelography
- more invasive than an MRI but gives excellent information regarding degrees of spinal cord compression
- useful in patients that cannot have an MRI (pacemaker), or have artifact (local hardware)
- contrast given via C1-C2 puncture and allowed to diffuse caudally, or given via a lumbar puncture and allowed to diffuse proximally by putting patient in trendelenburg position.
- Nerve conduction studies
- high false negative rate
- may be useful to distinguish peripheral from central process (ALS)
|
| Differential |
- Normal aging
- mild symptoms of myelopathy often confused with a "normal aging" process
- Stroke
- Movement disorders
- Vitamin B12 deficiency
- Amyotrophic lateral sclerosis (ALS)
- Multiple sclerosis
|
| Treatment |
- Nonoperative
- observation, NSAIDs, therapy, and lifestyle modifications
- indications
- mild disease with no functional impairment
- function is a more important determinant for surgery than physical exam finding
- patients who are poor candidates for surgery
- modalities
- medications (NSAIDS, gabapentin)
- immobilization (hard collar in slight flexion)
- physical therapy for neck strengthening, balance, and gait training
- traction and chiropractic modalities are not likely to benefit and do have some risks
- be sure to watch patients carefully for progression
- outcomes
- improved nonoperative outcomes associated with patients with larger transverse area of the spinal cord (>70mm2)
- some studies have shown improvement with immobilization in patients with very mild symptoms
- Operative
- surgical decompression, restoration of lordosis, stabilization
- indications
- significant functional impairment AND
- 1-2 level disease
- lordotic, neutral or kyphotic alignment
- techniques
- appropriate procedure depends on
- cervical alignment
- number of stenotic levels
- location of compression
- medical conditions (e.g., goiter)
- treatment procedures include (see below)
- anterior cervical diskectomy/corpectomy and fusion
- posterior laminectomy and fusion
- posterior laminoplasty
- combined anterior and posterior procedure
- cervical disk arthroplasty
- outcomes
- prospective studies show improvement in overall pain, function, and neurologic symptoms with operative treatment
- early recognition and treatment prior to spinal cord damage is critical for good clinical outcomes
|
| Techniques |
- Goals
- optimal surgical treatment depends on the individual. Things to consider include
- number of stenotic levels
- sagittal alignment of the spine
- degree of existing motion and desire to maintain
- medical comorbidities (eg, dysphasia)
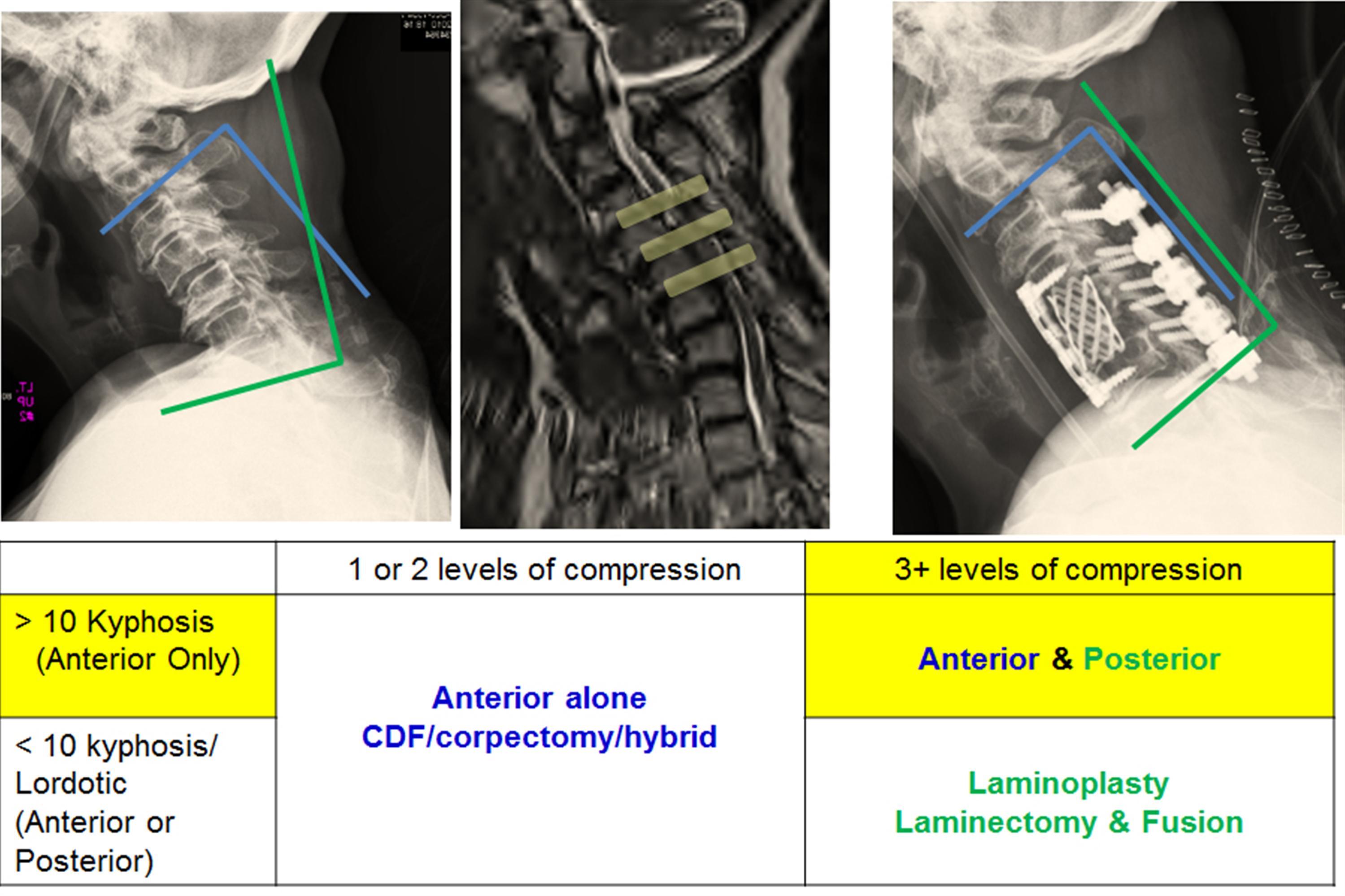
- simplified treatment algorithm
- Anterior Decompression and Fusion (ACDF) alone
- indications
- mainstay of treatment in most patients with single or two level disease
- fixed cervical kyphosis of > 10 degrees
- anterior procedure can correct kyphosis
- compression arising from 2 or fewer disc segments
- pathology is anterior (OPLL, soft discs, disc osteophyte complexes)
- approach
- uses Smith-Robinson anterior approach

- decompression
- corpectomy and strut graft may be required for multilevel spondylosis
- two level corpectomies tend to be biomechanically vulnerable (preferable to combine single level corpectomy with adjacent level diskectomy)
- 7% to 20% rates of graft dislodgement with cervical corpectomy with associated severe complications, including death, reported.
- fixation
- anterior plating functions to increase fusion rates and preserve position of interbody cage or strut graft
- pros & cons
- advantages compared to posterior approach
- lower infection rate
- less blood loss
- less postoperative pain
- disadvantages
- avoid in patients with poor swallowing function
- Laminectomy with posterior fusion
- indications
- multilevel compression with kyphosis of < 10 degrees
- > 13 degrees of fixed kyphosis is a contraindication for a posterior procedure
- in flexible kyphotic spine, posterior decompression and fusion may be indicated if kyphotic deformity can be corrected prior to instrumentation
- contraindications
- fixed kyphosis of > 10 degrees is a contraindication to posterior decompression
- will not adequately decompress spinal cord as it is "bowstringing" anterior
- pros & cons
- fusion may improve neck pain associated with degenerative facets
- not effective in patients with > 10 degrees fixed kyphosis
- Laminoplasty
- indications
- gaining in popularity
- useful when maintaining motion is desired
- avoids complications of fusion so may be indicated in patients at high risk of pseudoarthrosis
- contraindications
- cervical kyphosis
- > 13 degrees is a contraindication to posterior decompression
- will not adequately decompress spinal cord as it is "bowstringing" anterior
- severe axial neck pain
- is a relative contraindication and these patients should be fused
- technique
- volume of canal is expanded by hinged-door laminoplasty followed by fusion
- usually performed from C3 to C7
- open door technique
- hinge created unilateral at junction of lateral mass and lamina and opening on opposite side
- opening held open by bone, suture anchors, or special plates
- French door technique
- hinge created bilaterally and opening created midline
- pros & cons
- advantages
- allows for decompression of multilevel stenotic myelopathy without compromising stability and motion (avoids postlaminectomy kyphosis)
- lower complication rate than multilevel anterior decompression
- especially in patients with OPLL
- a motion-preserving technique
- pseudoarthrosis not a concern in patients with poor healing potential (diabetes, chronic steroid users)
- can be combined with a subsequent anterior procedure
- disadvantage
- higher avergae blood loss than anterior procedures
- postoperative neck pain
- still associated with loss of motion
- outcomes
- equivalent to multilevel anterior decompression and fusion
- Combined anterior and posterior surgery
- indications
- multilevel stenosis in the rigid kyphotic spine
- multi-level anterior cervical corpectomies
- postlaminectomy kyphosis
- Laminectomy alone
- indications
- rarely indicated due to risk of post laminectomy kyphosis
- pros & cons
- progressive kyphosis
- 11 to 47% incidence if laminectomy performed alone without fusion
|
| Complications |
- Surgical Infection
- higher rate of surgical infection with posterior approach than anterior approach
- Pseudoarthrosis
- incidence
- 12% for single level fusions, 30% for multilevel fusions
- treatment
- treat with either posterior wiring or plating or repeat anterior decompression and plating if patient has symptoms of radiculopathy
- Postoperative C5 palsy
- incidence
- reported to occur in ~ 4.6% of patients after surgery for cervical compression myelopathy
- no significant differences between patients undergoing anterior decompression and fusion and posterior laminoplasty
- occurs immediately postop to weeks following surgery
- mechanism
- mechanism is controversial
- in laminectomy patients, it is thought to be caused by tethering of nerve root with dorsal migration of spinal cord following removal of posterior elements
- prognosis
- patients with postoperative C5 palsy generally have a good prognosis for functional recovery, but recovery takes time
- Recurrent laryngeal nerve injury
- approach
- in the past it has been postulated that the RLN is more vulnerable to injury on the right due to a more aberrant pathway
- recent studies have shown there is not an increased injury rate with a right sided approach
- treatment
- if you have a postoperative RLN palsy, watch over time
- if not improved over 6 weeks than ENT consult to scope patient and inject teflon
- if you are performing revision anterior cervical surgery, and there is an any suspicion of a RLN from the first operation, obtain ENT consult to establish prior injury
- if patient has prior RLN nerve perform revision surgery on the same as the prior injury/approach to prevent a bilateral RLN injury
- Hardware failure and migration
- 7-20% with two level anterior corpectomies
- two level corpectomies should be stabilized from behind
- Postlaminectomy kyphosis
- treat with anterior/posterior procedure
- Postoperative axial neck pain
- Vertebral artery injury
- Esophageal Injury
- Dysphagia & alteration in speech
|








No comments:
Post a Comment